2418
Optimization of increasing signal-to-noise ratio (SNR) and contrast of black-blood T1-weighted images in carotid artery1Department of Radiological Service, Tokyo Women’s Medical University Yachiyo Medical Center, YACHIYO, Japan
Synopsis
We have developed a new black-blood imaging with radial scan (multi vane) method and improved motion sensitized driven equilibrium (iMSDE). In this study, we changed the following parameters [refocusing flip angle (RFA), TE prep, flow velocity encoding (VENC)]. In addition, we measured SNR and Contrast ratio (CR) to optimize image quality. As RFA increased in radial scan with iMSDE, SNR of muscle rose gently and CR increased. With the extension of TE prep, SNR of muscle declined and CR also declined. As VENC decreased, CR rose gently. There was a significant difference compared with the conventional method.
INTRODUCTION
Black blood imaging (BBI) is a technique to suppress blood signal, and is effective in increasing contrast between vessel wall and intravascular lesion such as plaque. Moreover, BBI method is able to reduce motion artifact due to pulsating blood. Therefore, BBI is effective in clinical medicine [1,2]. Recently, T1 turbo spin echo (TSE) method with a low variable refocusing flip angle (VRFA) is used for the carotid artery black-blood image. [3,4,5]. However, decreasing RFA decrease the signal-to-noise ratio (SNR) and T1 contrast. Therefore, we have developed a new black blood imaging with radial scan (multi vane) method and improved motion sensitized driven equilibrium (iMSDE) [6,7,8]. This method can get high SNR and high contrast because of high RFA, and can reduce motion artifact. [9,10,11,12].OBJECTIVE
Optimization of scan protocol for T1 black-blood images of carotid arteries with few artifacts and high SNR and high contrast.METHODS
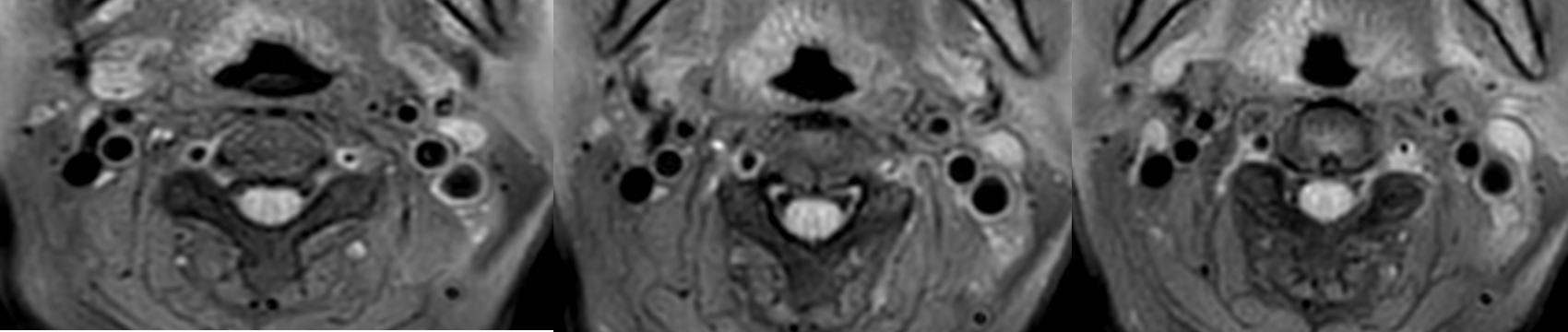
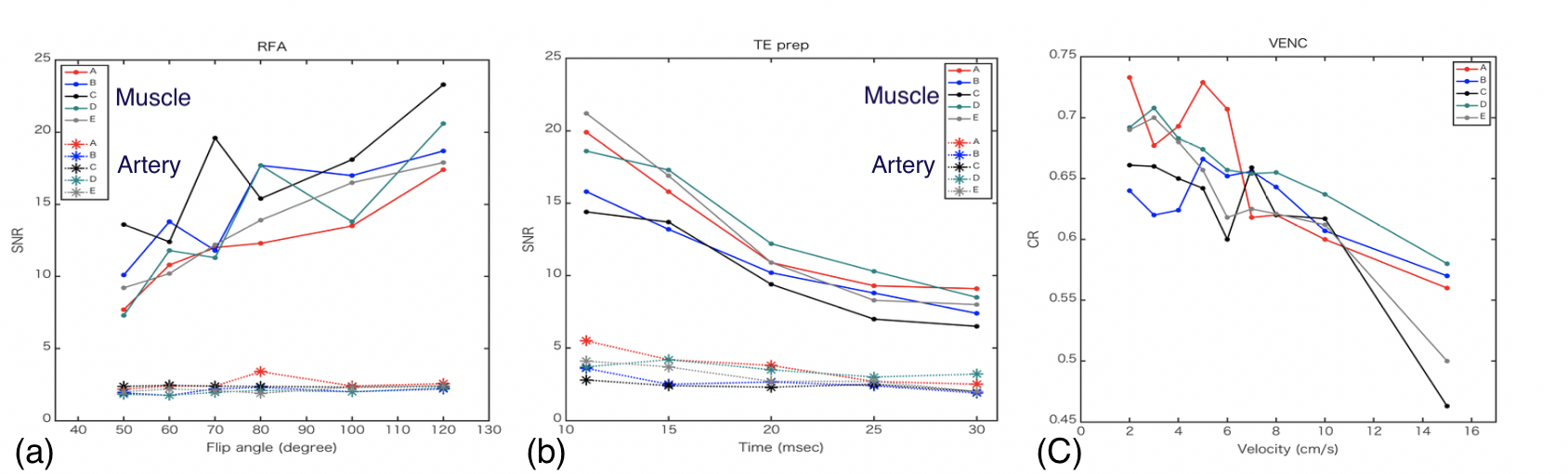
All examinations underwent MRI with a 3.0-T unit (Ingenia CX, Philips Medical Systems, the Netherlands) equipped with ds head neck coil, ds anterior coil, ds posterior coil. T1-weighted Black-blood images were obtained using iMSDE combined with radial scan (multi vane) (Fig. 1) and VRFA combined with TSE. However, black-blood T1-weighted images of VRFA combined with TSE has already been acquired for retrospective study. T1-weighted Black-blood images were acquired using radial scan with iMSDE (TR, 500ms; TE, 21ms; flip angle, 90degrees; field of view, 230 ×230mm2; matrix, 256 ×256; slice thickness, 3mm; slice gap, 0.3mm; acquisition time, 205s). In this study, we changed the following parameters (RFA, 50, 60, 70, 80, 100 and 120 degree; TE prep, 11, 15, 20, 25 and 30ms; flow velocity encoding (VENC), 2, 3, 4, 5, 6, 7, 8, 10 and 15 cm/s). In addition, we measured SNR and Contrast ratio (CR) to optimize image quality for T1-weighted Black-blood images. Furthermore, imaging of VRFA TSE was performed for comparison. Wilcoxon tests were used to assess the differences in SNR and CR between both black-blood T1-weighted images on the same patient. All statistical analyses were performed by using JMP (version 14.0 for Macintosh, SAS).Study population
Both volunteer and patient experiments were conducted with the approval of our Institutional ethics committee. 15 patients (13 men and 2 women; mean age, 52.9 years; age range, 38-76 years) suspected of having carotid artery disease underwent MRI including black-blood image of the carotid arteries. 5 volunteers 3 men and 2 women; mean age, 31.0 years; age range, 26-45 years) were control group.Image analyses
Regions of interest (ROI) were always placed in the sternocleidomastoid (SCM) muscle and carotid lumen. SNR was calculated by dividing the average signal intensity in the ROIs, which was set in the SCM muscle and carotid lumen, with the standard deviation of signal intensity in the ROI. Contrast ratios were calculated as follow; CR = (SCM muscle − carotid lumen) / (SCM muscle + carotid lumen).RESULTS
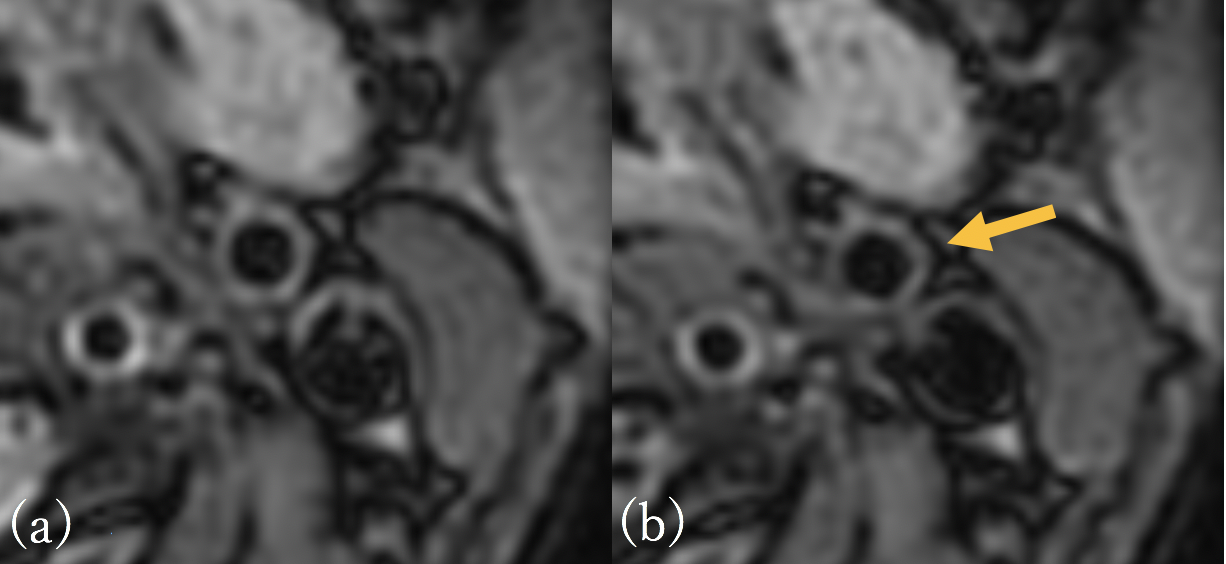
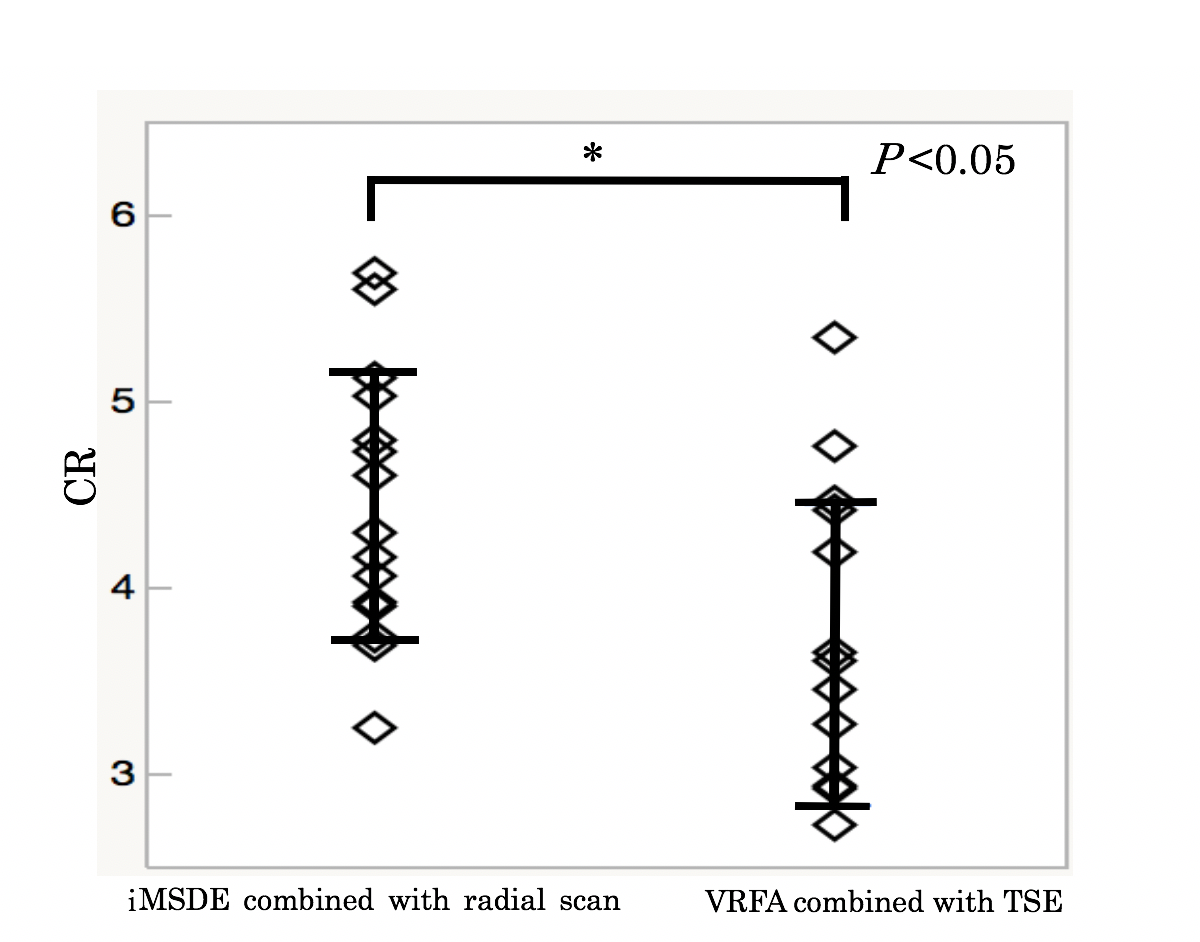
As RFA increased in radial scan with iMSDE, SNR of muscle rose gently and CR increased. With the extension of TE prep, SNR of muscle declined and CR also declined. As VENC decreased, CR rose gently (Fig. 2, 3). There was a significant difference compared with the conventional method (P<0.05. P=0.010) (Fig. 4, 5).CONCLUSION
Regarding with this study, we could obtain the better black-blood imaging which emphasizes T1 contrast when we set RFA was 120 degree, TE prep was 11ms, and VENC was 5-8 cm/s.Acknowledgements
No acknowledgement found.References
1, Urata T, et al. Nihon Hoshasen Gijutsu Gakkai Zasshi. 2012;68(7):871-9
2, Watanabe Y, et al. Neuroradiology. 2010; 52(4): 253-274
3, Xie Y, et al. Magn Reson Med. 2016 Jun;75(6):2286-94
4, Fan Z, et al. J Magn Reson Imaging. 2010 Mar;31(3):645-54
5, Yoneyama M, et al. Radiol Phys Technol. 2012 Jul;5(2):270-6
6, Nguyen TD, et al. J Magn Reson Imaging. 2008; 28(5): 1092-1100
7, Wang J, et al. J Magn Reson Imaging. 2010; 31(5): 1256-1263
8, Wang J, et al. Magn Reson Med. 2007; 58(5): 973-981
9, Schäffter T, et al. Magn Reson Med. 1999; 41(5): 954-963
10, Pipe JG, et al. Magn Reson Med. 1999; 42(5): 963-969
11, Forbes KP, et al. J Magn Reson Imaging. 2001; 14(3): 215-222
12, Hirokawa Y, et al. AJR Am J Roentgenol. 2008; 191(4): 1154-1158
Figures