2397
3D non-rigid motion correction for quantitative assessment of hepatic lesions with dynamic contrast enhanced MRI1Radiology, Charité Universitätsmedizin Berlin, Berlin, Germany, 2Physikalisch-Technische Bundesanstalt (PTB), Braunschweig and Berlin, Germany
Synopsis
Dynamic Contrast Enhanced (DCE) MRI of the liver is a powerful qualitative and quantitative clinical methodology used to identify lesions and characterize their functional behavior. Respiratory motion can lead to artefacts, impairing the calculation of contrast uptake curves and quantitative functional information. Here we present an approach, which provides non-rigid motion-corrected endothelial permeability (Ktrans) maps obtained from DCE images with temporal resolution of 6s and isotropic spatial resolution of 1.5mm3 acquired during free-breathing. The proposed framework was evaluated in 10 patients and led to an improved visualization of hepatic lesions and subsequent derivation of Ktrans maps.
Introduction
Dynamic contrast-enhanced (DCE) MRI is a clinical imaging modality using contrast agents to provide structural and functional information regarding tissue microvasculature. It is a widely used qualitative tool to identify healthy liver parenchyma and to determine the dignity of a lesion 1. In addition, it allows to calculate quantitative parametric maps describing endothelial permeability (Ktrans) by fitting of a pharmacokinetic model. A major challenge of quantitative and qualitative assessment is respiratory motion. Commonly breath-holding is used, yielding only a few data points in time (4-5) and leading to poor fitting accuracy. Respiratory motion compensation has been introduced in recent years, however these techniques usually have limited spatial resolution in the slice encoding direction (3-5 mm) and have not yet been assessed on the quantification of DCE parametric maps.2-6 Here we assess the effect of respiratory motion correction on endothelial permeability maps (Ktrans) obtained from DCE images with isotropic spatial resolution of 1.5mm3 and temporal resolution of 6s obtained during free-breathing.7 The approach is evaluated in 10 patients.Methods (Figure 1)
1.Data acquisition
Data was acquired continuously, for 5min with a 3D T1-weighted sequence (TE/TR/FA/FOV: 1.4/3.3ms/12°/280mm3) employing Golden Radial Phase Encoding (GRPE) sampling trajectory, during which contrast injection took place after 1min.
2.Motion estimation and Image reconstruction
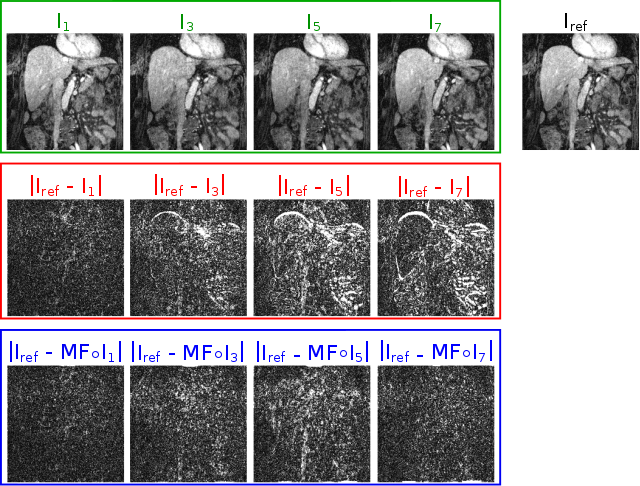
Data was retrospectively divided into 8 respiratory motion states that were estimated according to a respiratory self-navigator. Non-rigid respiratory motion fields were then obtained through registering these motion states to a reference state using a spline-based algorithm with a normalized mutual information metric. 8 Motion fields were used in a motion-corrected kt-SENSE image reconstruction framework to yield datasets with 48 dynamic phases (i.e. temporal resolution of 6s).9
3.Ktrans estimation
Image intensity values were converted to contrast agent concentration using a reference tissue method. 10 The hepatic artery was used as source of the input function. The resulting voxel-wise contrast uptake curves are fitted to the Extended Tofts’ Model in order to derive the Ktrans map 11:
$$C_{toi}(t) = v_{p}C_{p}(t) + K_{trans} \int_0^t C_{p}(\tau - \Delta T) e^{\frac{-K_{trans}}{v_{e}} (t - \tau - \Delta T)} d \tau$$
where Ctoi(t) represents the tissue contrast uptake curve in time, Cp(t) is the blood plasma contrast uptake curve measured in the hepatic artery, vp is the volume fraction of blood plasma, ve is the extravascular extracellular fractional volume, ΔT is the time delay of tissue enhancement relative to the dynamic contrast agent concentration in arterial plasma.
4.Experiments
The presented approach was applied to 10 patients (6 women; mean age 54.7±17.3years) undergoing whole-body PET-MR examinations on a 3T Biograph mMR. Patients with suspected or known hepatic lesions were injected with 0.025 mmol/kg of Gadoxetate disodium (Primovist) which is a hepatospecific gadolinium-based contrast agent, used exclusively in MRI liver imaging to assess the dignity of focal lesions. Patients undergoing examinations not related strictly or solely to liver imaging of metastases, were injected with 0.1 mmol/kg of Gadobutrol (Gadovist).
Results
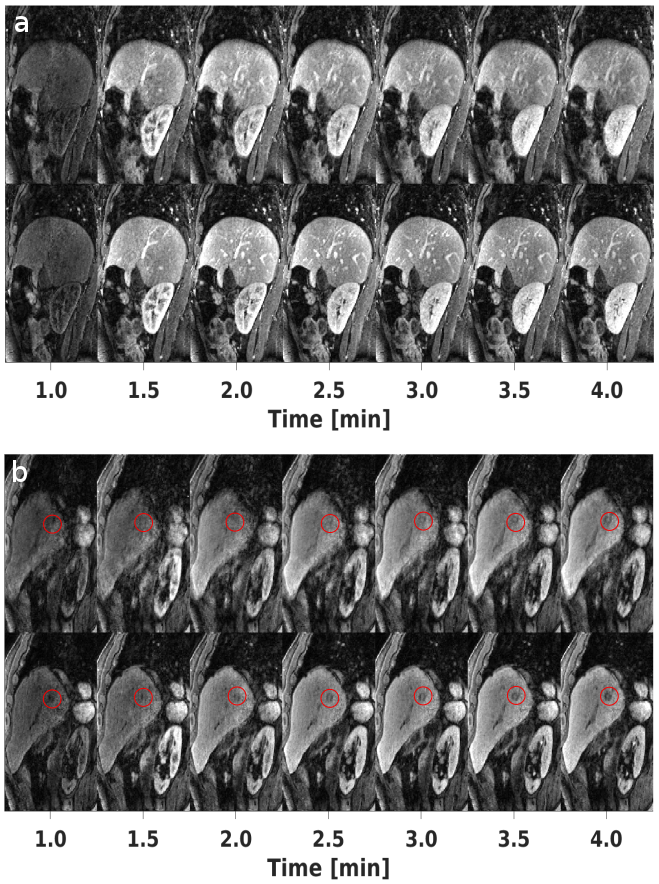
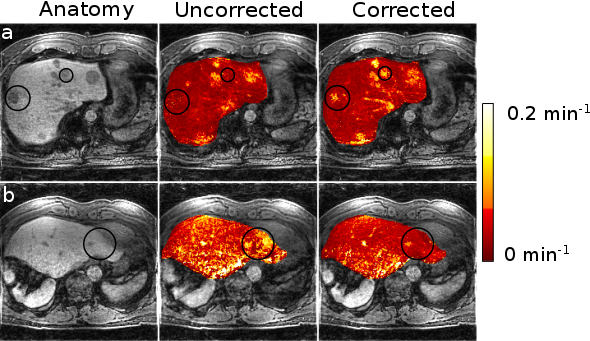
Respiratory resolved images are shown in Figure 2. Difference images before and after motion correction indicate accurate motion estimation. DCE images with and without motion correction are displayed in Figure 3. Corrected images have sharper edges and better-defined contrast of small features, such as lesions and vessels, compared to uncorrected images. Figure 4 shows the effect of respiratory motion on contrast uptake curves. The characteristic kinetic behavior of hepatic NET lesion with early contrast enhancement and early washout can be clearly seen in motion corrected images. Without motion correction, this characteristic temporal behavior is less pronounced. Respiratory motion has little effect on an input function obtained from the aorta (due to size and orientation). Motion correction strongly improves the input function calculated from the hepatic artery. Figure 5 shows two patients affected by neuro endocrine tumors (NET), with examples of lesions that are clearly seen in the Ktrans maps derived from motion corrected images but might be missed without motion correction.Conclusion
The proposed motion correction framework for quantitative DCE-MRI ensures accurate alignment between different dynamic images and minimizing respiratory motion artefacts which allows for accurate fitting of pharmacokinetic models. Respiratory motion correction leads to better lesions quantification in the Ktrans maps and more reproducible Ktrans values in healthy liver tissue, due to a more reproducible input function estimation. The high spatial resolution also allows for the calculation of the input function in small vessels, such as the hepatic artery, enabling more advanced models, e.g dual input single compartment model. 12,13Acknowledgements
Support of the German Research Foundation (DFG), project number GRK 2260, BIOQIC is acknowledged.References
- Choyke PL, Dwyer AJ, Knopp MV. Functional tumor imaging with dynamic contrast-enhanced magnetic resonance imaging. J Magn Reson Imag 2003;17:509–520.
- Bultman EM, Brodsky EK, Horng DE, et al. Quantitative hepatic perfusion modeling using DCE-MRI with sequential breath-holds. J Magn Reson Imaging 2014;39:853–865.
- Johansson A, Balter J, Cao Y. Rigid-Body Motion Correction of the Liver in Image Reconstruction for Golden-Angle Stack-of-Stars DCE MRI. Magn Reson Med 2018;79:1345–1353.
- Lin W, Guo J, Rosen MA, Hee KS. Respiratory motion-compensated radial dynamic contrast-enhanced (DCE)-MRI of chest and abdominal lesions. Magn Reson Med 2008;60:1135–1146.
- Johansson A, Balter J, Cao Y. Abdominal DCE-MRI reconstruction with deformable motion correction for liver perfusion quantification. Med Phys 2018;doi:10.1002/mp.13118.
- Fuin N, Catalano OA, Scipioni M, et al. Concurrent respiratory motion correction of abdominal PET and DCE-MRI using a compressed sensing approach. J Nucl Med 2018;https://doi.org/10.2967/jnumed.117.203943.
- Ippoliti M, Makowski M, Schaeffter T, Kolbitsch C. 3D non-rigid motion corrected dynamic contrast enhanced MRI of the liver with high isotropic spatial resolution. In: Proceedings of Joint Annual Meeting ISMRM-ESMRMB, Paris, France. ; 2018:476.
- Rueckert D, Sonoda LI, Hayes C, Hill DLG, Leach MO, Hawkes DJ. Nonrigid registration using free-form deformations: application to breast MR images. IEEE Trans Med Imaging 1999;18:712–721.
- Cruz G, Atkinson D, Buerger C, Schaeffter T, Prieto C. Accelerated motion corrected three-dimensional abdominal MRI using total variation regularized SENSE reconstruction. Magn Reson Med 2016;75:1484–1498.
- Medved M, Karczmar G, Yang C, et al. Semiquantitative analysis of dynamic contrast enhanced MRI in cancer patients: variability and changes in tumor tissue over time. J Magn Reson Imaging 2004;20:122–128.
- Tofts PS, Brix G, Buckley DL, et al. Estimating kinetic parameters from dynamic contrast-enhanced T(1)-weighted MRI of a diffusable tracer: standardized quantities and symbols. J Magn Reson Imaging 1999;10:223–232.
- Jajamovic GH, Calgano C, Dyvorne HA, Rusinek H, Taouli Bachir. DCE-MRI of the liver: Reconstruction of the Arterial Input Function Using a Low Dose Pre-Bolus Contrast Injection. PLoS One 2014;9:e115667.
- Materne R, Smith AM, Peeters F, et al. Assessment of hepatic perfusion parameters with dynamic MRI. Magn Reson Med 2002;47: 135–142.
Figures