2387
Statistical prediction of recurrence-free survival at 10 years in breast cancer patients1Stony Brook University, Stony Brook, NY, United States
Synopsis
This study examined whether axillary lymph-node size accurately predicts or improves prediction of 10-year recurrence-free survival. We found that for single-variable analysis, the top predictor of recurrence-free survival was pre-neoadjuvant chemotherapy (NAC) nodal volume (AUC=0.67), followed by pre-NAC tumor volume (AUC=0.66). In 4-variable analysis, the top set of predictors was pre-NAC nodal volume, human epidermal growth factor receptor 2 (HER2) positivity, pre-NAC tumor volume, and tumor volume difference between pre- and early-NAC time points (AUC=0.79). This is the first study of investigating prediction performance of recurrence-free survival using longitudinal volume change of axillary lymph-node volume in breast cancer patients.
Introduction
Breast cancer is most concerning when it metastasizes to the axillary lymph nodes (aLN) because it could lead to distant metastasis [1]. aLN data could thus offer prognostic value for recurrence free survival (RFS). Although previous studies have examined the ability of tumor volume by MRI, pathological complete response (PCR), and receptor subtypes to predict RFS in breast cancer patients, RFS prediction accuracy is controversial with some studies found reasonable accurate prediction of RFS while others found no association [2-5]. The ability of longitudinal measurement of aLN size to predict RFS however has not been investigated. One possible reason is that MRI of aLNs have limited resolution and contrast. The goal of this study was thus to examine whether aLN volume derived from MRI accurately predicts RFS, and whether the addition of aLN size helps to improve RFS prediction performance.Methods
A subset of stage-2 or 3 breast-cancer patients from ISPY-1 clinical trial which had “usable” aLN MRI and 10-year RFS were analyzed [5]. MR images were from 1.5T scanner using a standard breast coil. The image used for segmentation of aLNs was the 3D high-resolution T1-weighted first post-contrast image. Given this was a multicenter trial, resolution varied slightly, but was approximately 0.7 x 0.7 x 2 mm. The total sample size was 92 patients that had aLN volume (aLNV), tumor volume (TV), and RFS data at the pre-neoadjuvant chemotherapy (NAC) time point 1 (tp1), tp2, tp3 and post-NAC tp4. For consistency, the largest node pre-NAC per patient was contoured on DCE MRI under guidance of radiologists. Retrospective review by our breast radiologists confirmed all (95%) of the largest aLNs were the most suspicious of malignancy. Large aLN volume was defined by using a threshold of 3 mL (1.79 cm in diameter), which was 4.5 times the standard deviation of the average unaffected node volume (obtained from 198 nodes from 62 participants). Tumor volume was determined by a percent enhancement threshold method [5].
Receiver operating curve (ROC) analysis was performed for the following parameters with respect to RFS prediction: a) large versus small aLN volume, b) enhancing tumor volume at different time points before, during and after NAC, c) three different hormone receptor subtype categories (hormone receptor (HR)+/ human epidermal growth factor receptor 2 (HER2)-, HER2+ and triple negative (TN)) and d) full, breast, and nodal PCR. Area under the curve (AUC), sensitivity, specificity and accuracy were tabulated. A univariate and multivariate analysis was performed. A P-value of 0.05 was used to determine statistical significance.
Results
In the single-variable analysis, the top predictors (largest AUC) of RFS were: i) pre-NAC aLNV, ii) pre-NAC TV, iii) Nodal PCR, and iv) post - pre-NAC TV. In the two-variable analysis, the top two combinations were: i) Nodal PCR +pre-NAC TV, and ii) pre-NAC aLNV + pre-NAC TV. In the three-variable analysis, the top two combinations were: i) pre-NAC aLNV + Nodal PCR + pre-NAC TV, and ii) pre-NAC aLNV + pre-NAC TV + (tp2 - pre-NAC TV).Discussion
Whether it is univariate or multivariate predictive model, nodal volume and/or nodal PCR was amongst the top predictors of RFS. The highest AUC was the four-variable predictors: nodal volume, HER2 positivity, tumor volume, and the tumor volume difference between tp2 and tp1 (AUC=0.79). These findings support the notion that nodal information (nodal PCR and nodal volume) is highly predictive of RFS. This is not unexpected because distant metastasis stems largely from axillary lymph node and is linked to RFS. Our results were overall more favorable compared to a previous study using ISPY-1 dataset Level 3 ISPY-1 data set (N=162) [5] (our dataset is a subset because not all patients had “usable” nodal MR images). In their study, the top predictor of single variable was residual cancer burden class or tumor volume at tp2 with AUC of 0.67 and the top predictor of 4-variable included functional volume differences, residual cancer burden, and HR+/HER2- receptor subtype category (AUC=0.72). A likely explanation for such discrepancy could be in part due to the inclusion of aLN volume.Conclusions
We found that aLN size per se is highly predictive of RFS at 10 years in breast-cancer patients. The addition of aLN volume augmented prediction performance of RFS. To our knowledge, this is the first study of investigating the prediction performance of RFS using longitudinal axillary lymph node size in breast cancer patients.Acknowledgements
No acknowledgement found.References
[1] Jatoi I et al. Significance of axillary lymph node metastasis in primary breast cancer. J Clin Oncol. 1999 Aug;17(8):2334-40.
[2] Partridge SC et al. MRI measurements of breast tumor volume predict response to neoadjuvant chemotherapy and recurrence-free survival. AJR Am J Roentgenol. 2005 Jun;184(6):1774-81.
[3] Esserman LJ et al. Pathologic complete response predicts recurrence-free survival more effectively by cancer subset: results from the I-SPY 1 TRIAL--CALGB 150007/150012, ACRIN 6657. J Clin Oncol. 2012 Sep 10;30(26):3242-9. doi: 10.1200/JCO.2011.39.2779. Epub 2012 May 29.
[4] Loo CE et al. Survival is associated with complete response on MRI after neoadjuvant chemotherapy in ER-positive HER2-negative breast cancer. Breast Cancer Res. 2016 Aug 5;18(1):82. doi: 10.1186/s13058-016-0742-0.
[5] Hylton NM et al. Neoadjuvant Chemotherapy for Breast Cancer: Functional Tumor Volume by MR Imaging Predicts Recurrence-free Survival-Results from the ACRIN 6657/CALGB 150007 I-SPY 1 TRIAL. Radiology. 2016 Apr;279(1):44-55. doi: 10.1148/radiol.2015150013. Epub 2015 Dec 1.
Figures
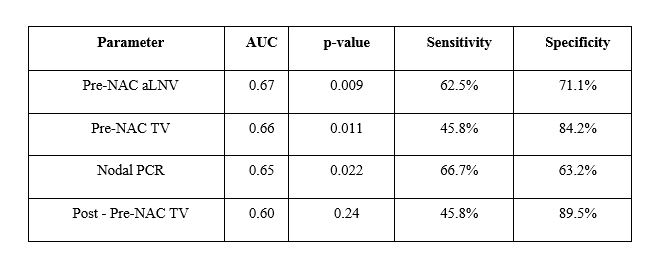
Table 1. Single parameter prediction of recurrence-free survival
AUC: area under the curve, PCR: pathological complete response, NAC: neoadjuvant chemotherapy, aLNV: axillary lymph node volume, TV: tumor volume
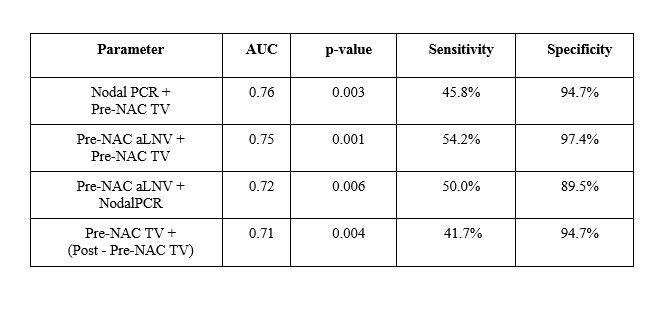
Table 2. Two-parameter prediction of recurrence-free survival
AUC: area under the curve, PCR: pathological complete response, NAC: neoadjuvant chemotherapy, aLNV: axillary lymph node volume, TV: tumor volume
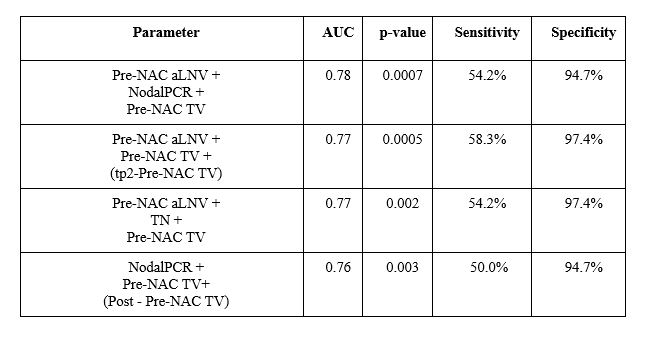
Table 3. Three-parameter prediction of recurrence-free survival
AUC: area under the curve, TN: triple negative, PCR: pathological complete response, NAC: neoadjuvant chemotherapy, tp: time point, aLNV: axillary lymph node volume, TV: tumor volume
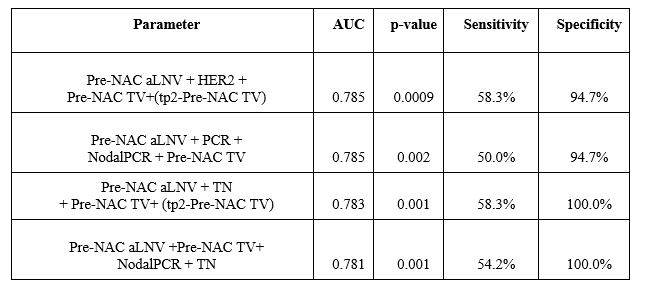
Table 4. Four-parameter prediction of recurrence-free survival
AUC: area under the curve, TN: triple negative, HER2: human epidermal growth factor receptor 2, PCR: pathological complete response, NAC: neoadjuvant chemotherapy, tp: time point, aLNV: axillary lymph node volume, TV: tumor volume