2385
Feasibility of Magnetic Resonance Fingerprinting of Glioblastoma Multiforme1Department of Radiology, University of Cambridge, Cambridge, United Kingdom, 2Cancer Research UK, Cambridge, United Kingdom, 3IMAGO7 Foundation, Pisa, Italy, 4GE Healthcare, Munich, Germany
Synopsis
Magnetic Resonance Imaging (MRI) research seeks to establish fast, sensitive, repeatable, and quantitative methods. The reduction of MRI acquisition times is important for patients who have significant disease, such as glioblastoma multiforme (GBM), and therewith difficulties with lengthy scan sessions. Magnetic Resonance Fingerprinting (MRF) is a method that can enable fast quantitative T1 and T2 mapping by exploiting transient signals caused by the variation of pseudorandom sequence parameters. This work demonstrates the feasibility of MRF in three patients with GBM, showing two before and after gadolinium contrast.
Introduction
Magnetic Resonance Imaging (MRI) research seeks to establish fast, sensitive, repeatable, and quantitative methods. Standard clinical MRI often only obtain contrast-weighted images, resulting in a semi-quantitative outcomes that can reduce inter-site repeatability of MRI techniques [1]. Quantitative MRI promises to improve the repeatability and reproducibility of MRI, however, quantitative methods are traditionally slow or subject to inaccuracies from field inhomogeneities. The reduction of MRI acquisition times is important for patients who have significant disease, such as glioblastoma multiforme (GBM), and therewith difficulties with lengthy scan sessions [2]. Magnetic Resonance Fingerprinting (MRF) is a method that can enable fast quantitative T1 and T2 mapping by exploiting transient signals caused by the variation of pseudorandom sequence parameters [2-4].Methods
This work investigates the feasibility of MRF in three patients with GBM, with and without gadolinium contrast. Three participants with GBM were imaged on a 3.0 T MRI system (MR750 GE Healthcare, Waukesha, WI, USA) using a 12-channel receive-only head coil. Imaging occurred with local ethical approval. The MR protocol consisted of standard clinical sequences, followed by gadolinium contrast. All three subjects had MRF performed without contrast, and two of the subjects had MRF performed after contrast. The MRF acquisition consisted of a 5min20sec 2D steady-state-free-precession (SSFP) sequence [3,4], with 979 frames using under-sampled spirals interleaved by golden-angle. Imaging parameters were: field-of-view = 205x205mm2, matrix = 256x256, slices = 24, slice thickness = 3.0mm, spacing 1.0mm, sampling bandwidth = ±250kHz, slice dephasing = 8π, echo time = 2.5ms, with repetition time and flip angle lists matching the values in Jiang [3]. The maximum gradient strength per spiral was 35mT/m and the maximum slew rate was 137T/m/s. Quantitative MRF T1 and T2 maps were obtained by pattern matching of T1 and T2 simulation dictionary with reconstructed time frames of the acquired data. The MRF dictionary was computed for T1 and T2 using the extended phase graphs formalism [4] and included the slice profile [5]. Regions-of-interest (ROIs) for analysis were collected on 4-5 slices over a large tumour-containing region. Similar ROIs were used for pre and post contrast analysis.Results
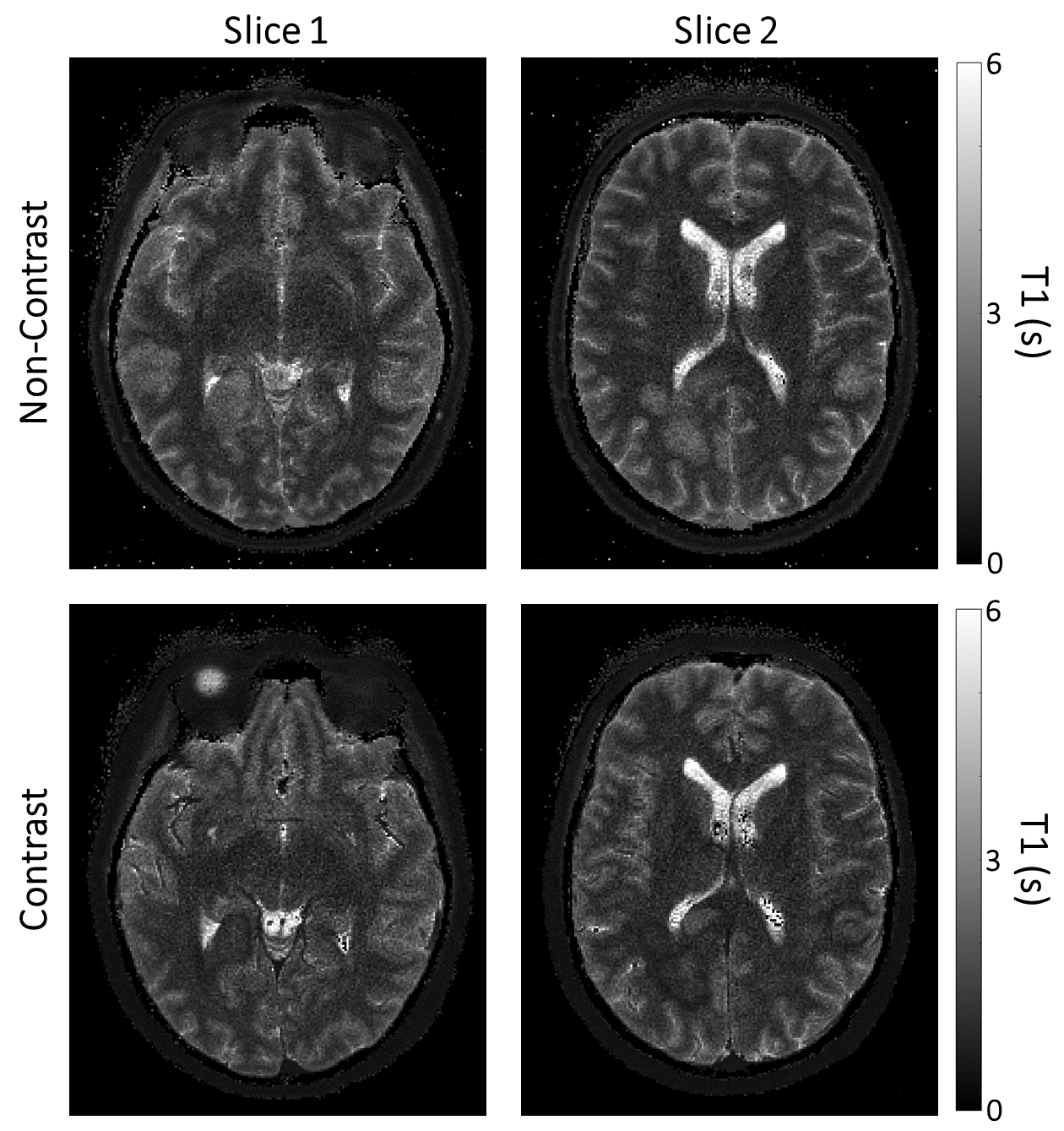
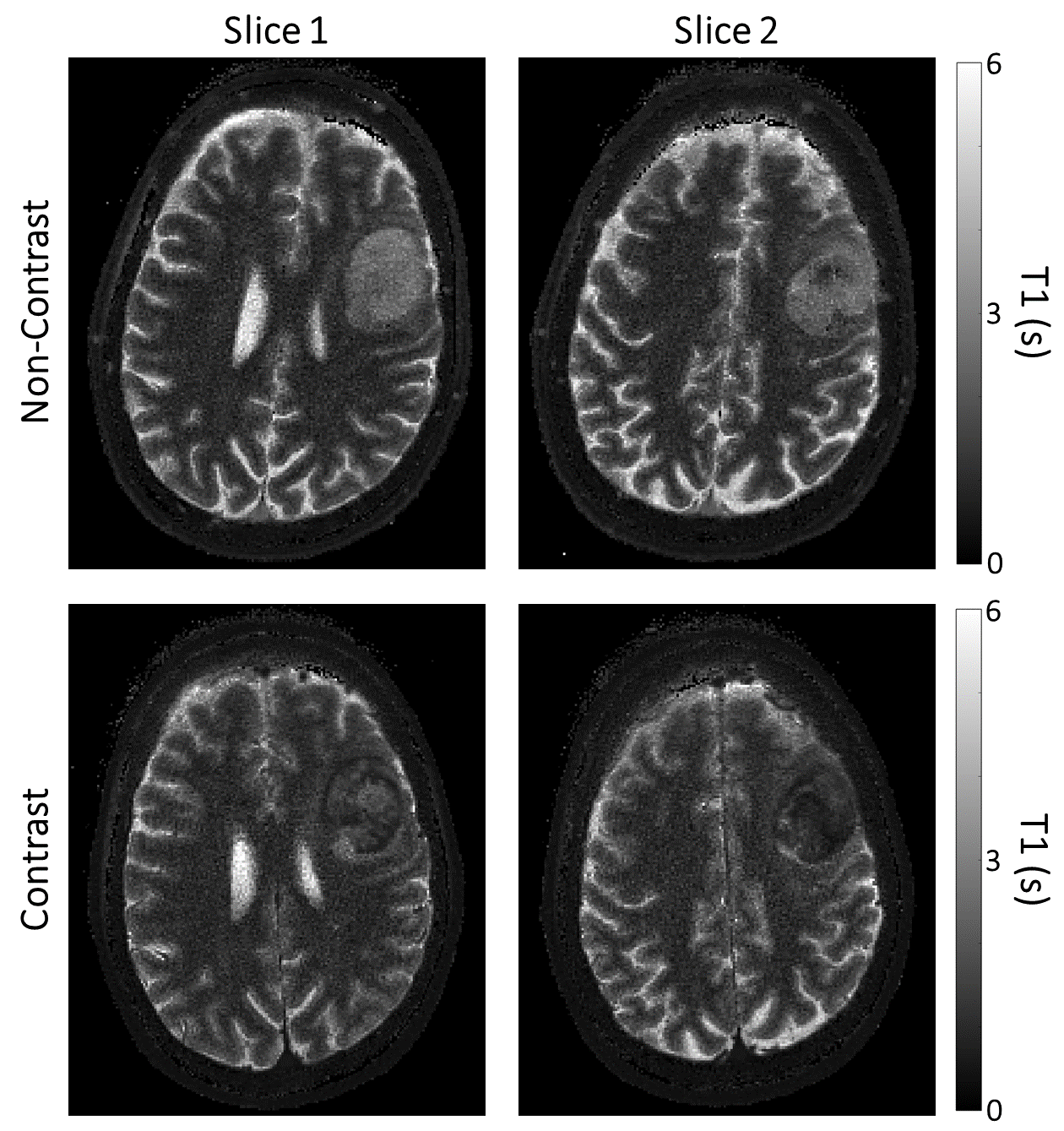
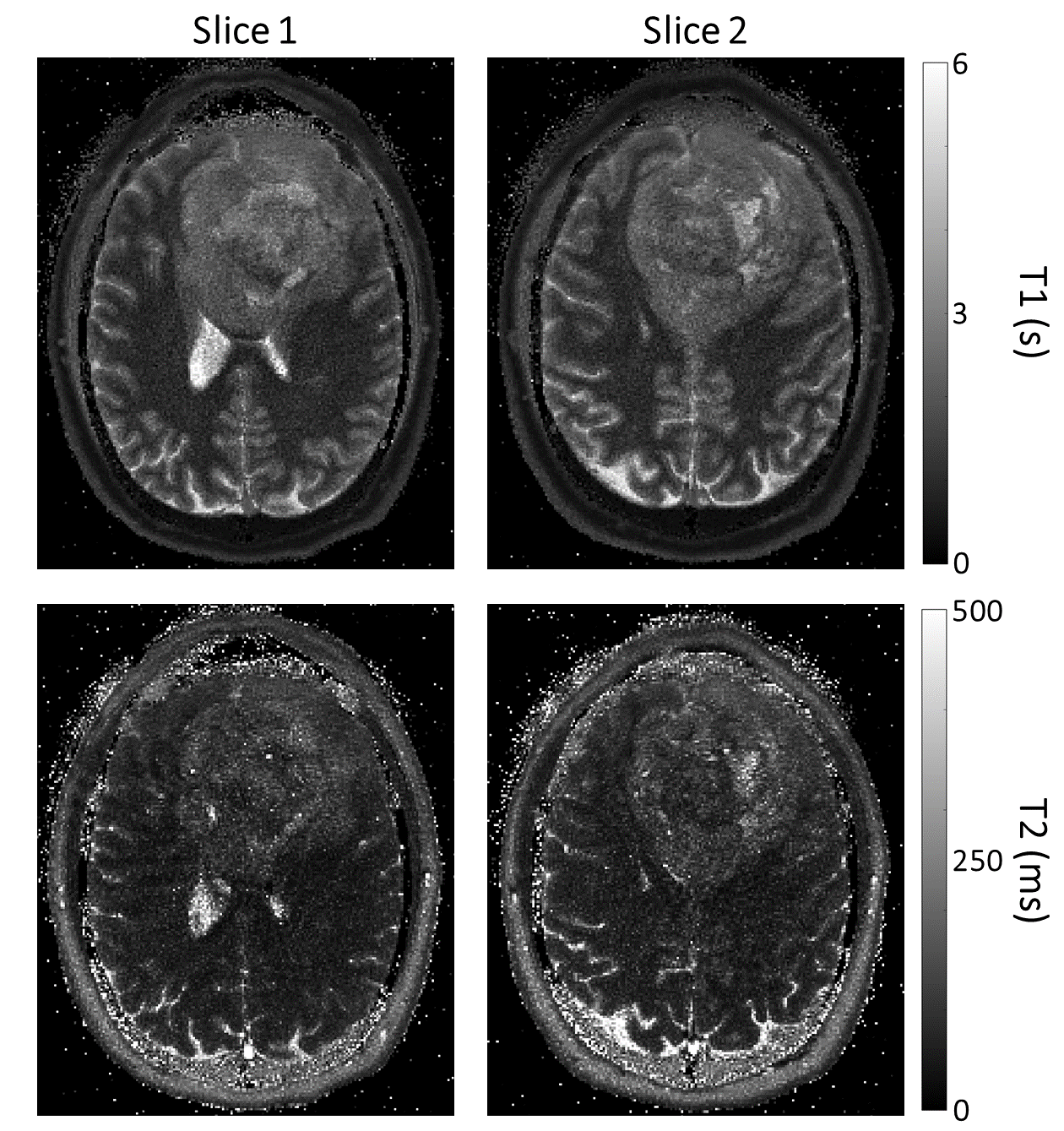
The T1 and T2 maps generated from MRF are shown in Figures 1-3. Estimated means and standard deviations for T1 and T2 are presented Table 1. The ratio of pre to post contrast values in both tumours for T1 was 1.83-1.87 and for T2 was 0.94-1.09.Discussion
This feasibility study of MRF with and without contrast enhancement proved successful in obtaining resolutions that could be clinically feasible (0.8x0.8mm2), with fully quantitative rather than semi-quantitative measurements. MRF has demonstrated evidence of accuracy for long T1 values (>1 second) [6], which may improve tumour characterisation through T1 values. Heterogeneity of the T1 and T2 maps can be observed, which may help in distinguishing different GBM types and in determining a suitable treatment strategy. The use of gadolinium contrast with MRF for investigating GBMs is novel to this work. Gadolinium contrast is used for many diagnostic MRI applications, despite concerns about gadolinium retention in deep grey matter structures, especially in patients undergoing radiation therapy2. If MRF or other multi-parametric methods prove successful in improving the sensitivity of contrast-enhanced MRI, then they could result in a reduced amount of contrast used clinically, which would be safer for the patient.Conclusion
This work demonstrates fast quantitative T1 and T2 mapping of the brain using MR Fingerprinting in patients with GBM. The T1 within areas of the glioblastomas was shortened by roughly 50% by gadolinium . The potential benefit of MRF is that it could result in fast, accurate, quantitative MRI that could be used for reliable follow-up and treatment response monitoring.Acknowledgements
This work has been supported by Cancer Research UK, and the CRUK & Engineering and Physical Sciences Research Council (EPSRC) Cancer Imaging Centre in Cambridge and Manchester. JDK and DAK are supported by GlaxoSmithKline.
Additional support has been provided by the CRUK Cambridge Centre, the National Institute of Health Research (NIHR), Cambridge Biomedical Research Centre and Addenbrooke’s Charitable Trust.
References
1. Lim, W. H. et al. Does radiation therapy increase gadolinium accumulation in the brain?: Quantitative analysis of T1 shortening using R1 relaxometry in glioblastoma multiforme patients. PLoS One 2018;13:1–14 .
2. Badve, C., Yu, A., Dastmalchian, S., Rogers, M., Ma, D., Jiang, Y., Margevicius, S., Pahwa, S., Lu, Z., Schluchter, M. and Sunshine, J. MR fingerprinting of adult brain tumors: initial experience. American Journal of Neuroradiology, 2017;38(3):492-499.
3. Ma D, Gulani V, Seiberlich N, Liu K, Sunshine JL, Duerk JL, et al. Magnetic resonance fingerprinting. Nature. 2013;495(7440):187-92.
4. Jiang Y, Ma D, Seiberlich N, Gulani V, Griswold MA. MR fingerprinting using fast imaging with steady state precession (FISP) with spiral readout. Magnetic Resonance in Medicine. 2015;74(6):1621-31.
5. Buonincontri, G., Sawiak, S.J., 2016. MR fingerprinting with simultaneous B1 estimation. Magnetic Resonance in Medicine 76:1127-1135.
6. Jiang, Y., Ma, D., Keenan, K.E.,
Stupic, K.F., Gulani, V. and Griswold, M.A.. Repeatability of
magnetic resonance fingerprinting T1 and T2 estimates assessed using the
ISMRM/NIST MRI system phantom. Magnetic Resonance in edicine, 2017;78(4):1452-1457.
Figures