2380
Molecular MRI differentiation between thyroid papillary carcinoma and thyroid adenoma without cystic degeneration using endogenous protein-based Amide Proton Transfer Signals1Department of Radiology, Guangdong Second Provincial General Hospital, guangzhou, China, 2Philips Healthcare,Guangzhou, China, guangzhou, China
Synopsis
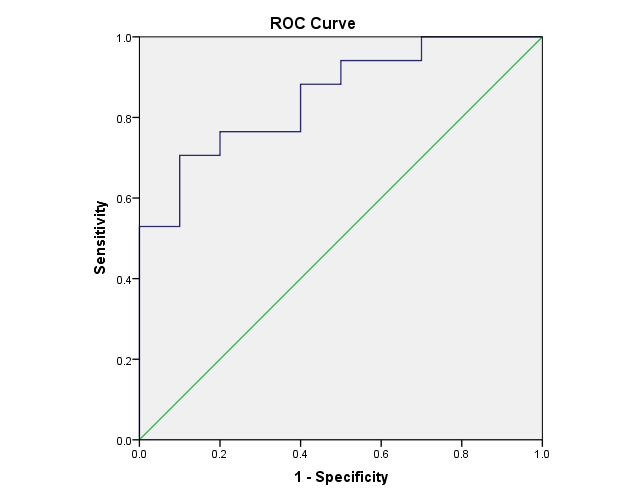
To identify thyroid papillary carcinoma from thyroid adenoma, we acquired amide proton transfer(APT) value of the both by using the 3T MRI. The differences of APT value of the both were statistically compared by means of nonparametric methods and receiver operating characteristic (ROC) curve analyses were used. The results showed statistical differences among the two nodules, suggesting that APTw imaging can be considered for differentiation of thyroid carcinoma from benign thyroid carcinoma.
Purpose
Thyroid nodules are a common clinical problem. Epidemiologic studies have shown that the prevalence of palpable thyroid nodules was accounted for approximately 5% in women and 1% in men1 living in iodine-sufficient parts of the world. Thyroid nodules are abnormal growths located on the thyroid gland. In case thyroid nodules are benign, like the thyroid adenoma, the first thing a doctor will recommend is to watch the way the nodules evolve. In the cases in which the thyroid nodules formed are cancerous, like the thyroid papillary carcinoma, the most common treatment involves surgery. Differention thyroid cancer from benign nodules is becoming increasingly prevalent. Amide proton transfer weighted(APTW) imaging can generate molecular MRI signals that are based on the amide protons of endogenous mobile proteins and peptides. This study aimed to investigate the feasibility of this new imaging method on the thyroid gland tissue by using the 3T MRI, and its role on differentiating thyroid papillary cancer from thyroid adenoma for better clinical management.Methods
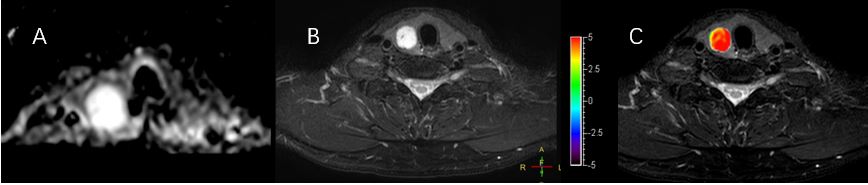
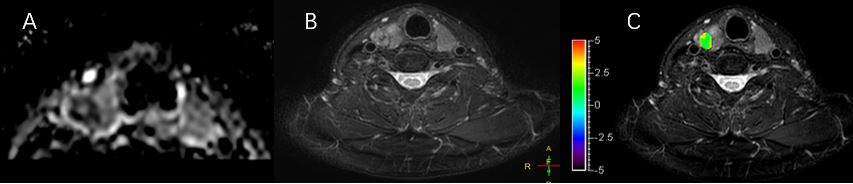
Twenty-six patients who signed informed consent were recruited, including 17 thyroid adenoma patients and 10 thyroid papillary carcinoma patients. Patients had no clinical history of previous surgery, corticosteroid administration, chemotherapy, or radiotherapy. MRI studies were performed using a 3.0 T system (Ingenia, Philips, the Netherlands) with a 25-channel head-neck coil. APT imaging was performed using a three-dimensional (3D) turbo-spin-echo Dixon sequence with imaging parameters as follows: acquisition voxel size of 1.8 × 1.8 mm, slice thickness of 4.4 mm, repetition time (TR)/echo time (TE) of 4108 ms/5.9 ms, turbo spin echo factor of 158; total slice of 10 to cover the entire lesions. seven saturation frequency offsets (±3.5, ±3.42, ±3.58 ppm and 1540ppm) were adapted with four repetitions at ±3.5 ppm to attain a sufficient signal-to-noise ratio (SNR) within an appropriate clinical time frame. Saturation RF pulses for APT imaging were implemented with an amplitude of 2 μT and duration of 2 seconds. B0 maps were obtained with three acquistions at 3.5ppm of different TEs. B0 corrected ATPw images were reconstructed online. A 2D region of interest (ROI) was visually placed over each solid nodule for each patient and then the mean APTW value were recorded for each ROI. To assess such molecular information differences between thyroid carcinoma and thyroid adenoma, nonparametric methods and receiver operating characteristic (ROC) curve analyses were used.Results and Discussion
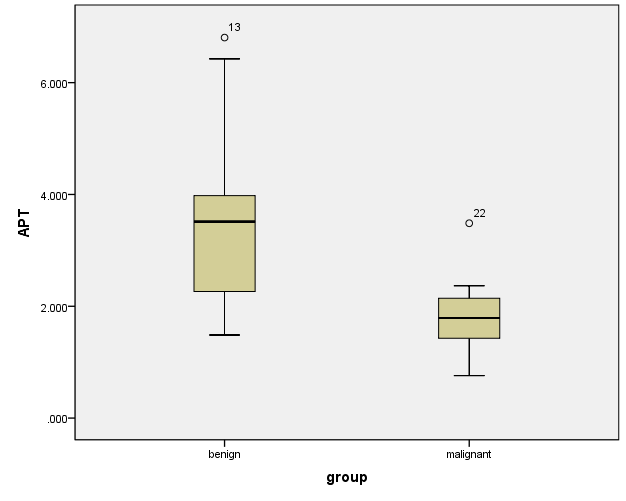
APTW value of thyroid carcinoma was significantly lower than thyroid adenoma. The result was connected with abundant thyroid colloid retention on thyroid adenoma (Fig. 3). On the contrary, thyroid carcinoma, a slow-growing tumor, usually was small size lesion without abundant thyroid colloid. So there was a big difference between thyroid adenoma and thyroid carcinoma.
Conclusion
APTw imaging can be considered for differentiation of thyroid carcinoma from benign thyroid carcinoma.Acknowledgements
This work was supported by Department of Radiology, Guangdong Second Provincial General Hospital and Philips Healthcare, Guangzhou, China.References
1.Bryan R. Haugen,1,* Erik K. Alexander,2 Keith C. Bible, 2015 American Thyroid Association ManagementGuidelines for Adult Patients with Thyroid Nodulesand Differentiated Thyroid Cancer.Figures