2377
The value of 1.5T contrast-enhanced T1 SPACE sequence in the simulation and planning for Cyberknife stereotactic radiosurgery of brain metastases: patient positioning accuracy, lesion detectability, and target delineation reliability1Medical Physics and Research Department, Hong Kong Sanatorium & Hospital, Happy Valley, Hong Kong, 2Department of radiotherapy, Hong Kong Sanatorium & Hospital, Happy Valley, Hong Kong, 3Department of Diagnostic and Interventional Radiology, Hong Kong Sanatorium & Hospital, Happy Valley, Hong Kong
Synopsis
Stereotactic radiosurgery (SRS) is increasingly used for multiple brain metastases (BM) treatment and imposes critical requirements on the accuracy of BM detection, localization and definition in the treatment planning. SPACE sequence is valuable in BM detection for diagnosis, while its value in the BM SRS planning has rarely been explored. We prospectively and quantitatively assessed CE-T1-SPACE in the treatment simulation and planning of Cyberknife-guided BM SRS on a 1.5T MRI-simulator. The results showed that CE-T1-SPACE facilitated high patient positioning accuracy, superior BM detectability and reliable GTV delineation, showing great value in the treatment planning of BM SRS.
INTRODUCTION
Stereotactic radiosurgery (SRS) is increasingly used for the treatment of patients with multiple brain metastases (BM) to achieve better local control while minimize cognitive effects associated with whole brain radiotherapy (WBRT) (1). SRS imposes critical requirements on the accuracy of BM detection, localization and definition in the treatment planning. Variable flip angle fast spin echo sequence, e.g. SPACE on Siemens MRI, has been proven valuable in brain metastases diagnosis, especially in its superior lesion detectability performance over conventional sequences (2), e.g. MP-RAGE, while its value in the treatment planning of BM SRS has rarely been explored. In this study, we aimed to prospectively assess the value of contrast-enhanced (CE) T1-SPACE in the treatment simulation and planning of a frameless BM Cyberknife® (Accuracy Inc, Sunnyvale, CA, USA) SRS by using a 1.5T MRI-simulator in terms of patient positioning accuracy, lesion detectability and gross target volume (GTV) delineation reliability.METHODS
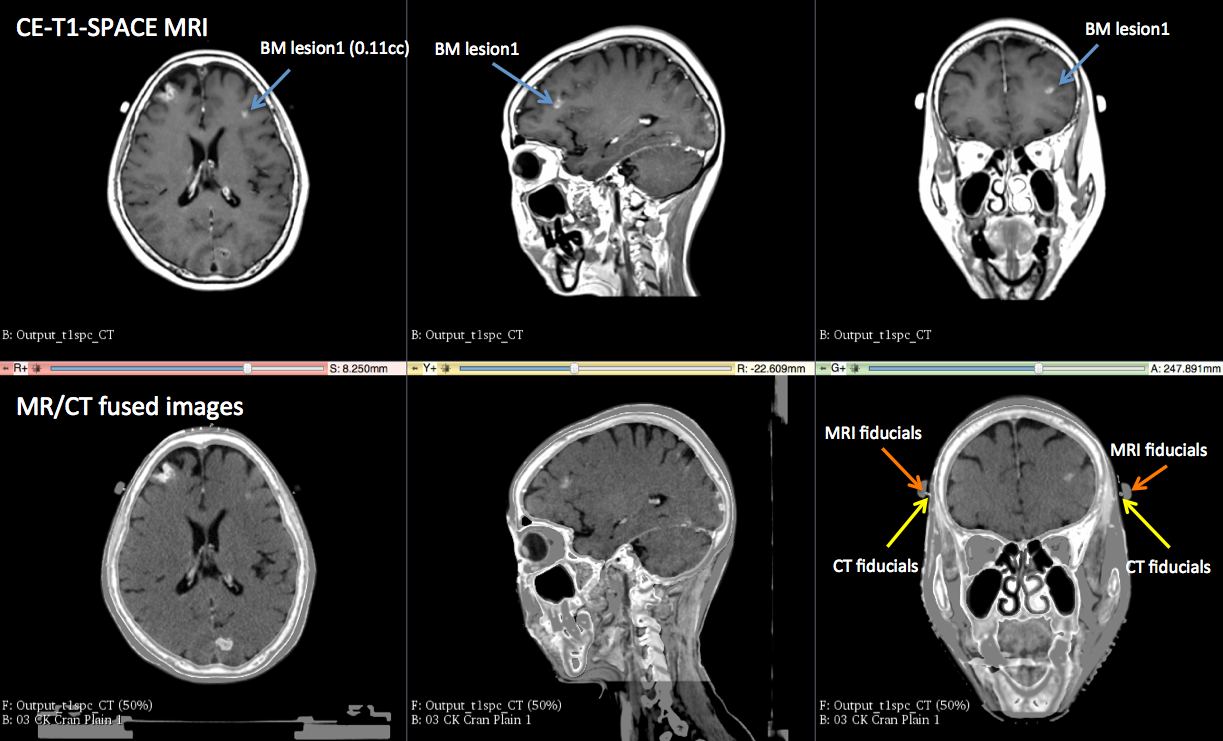
16 clinically-confirmed BM patients (61.5±11.1 years) received MR-simulation scan (GADOVIST® 0.1mmol/kg contrast-enhanced CE 3D-T1-SPACE: TE/TR=7.2/420ms; ETL=40; GRAPPA=2; BW=650Hz/pixel; voxel-size=1x1x1mm3; duration=4min24sec; 3D-geometric-correction=ON) on a 1.5T MR-simulator (Aera, Siemens Healthineers, Erlangen, Germany) scans in the identical thermoplastic mask fixed treatment position after their CT-simulation on the same day prior to their Cyberknife SRS. Rigid MRI/CT registration based on mutual information maximization was conducted. Fiducial markers and anatomical point landmarks were used to assess the MRI-simulation patient positioning accuracy. BM lesions were blindly contoured twice on MRI fused CT images by an over-10year-experienced observer. Number, center position, volume, average Hausdorff distance, dice similarity coefficient (DSC) of the contoured lesions were quantified to assess detectability and GTV delineation reliability.RESULTS
MR-simulation scan was successfully completed in all patients. CE-T1-SPACE image quality was evaluated as excellent by MRI physicists, radiologists and oncologists. Totally 56 BM were detected (volumes: 1.90±5.80 cc, ranged from 0.008-33.78 cc) utilizing the high isotropic MR resolution with small partial volume effect. The position differences of fiducial markers and anatomical landmarks between registered MRI/CT images were mostly sub-millimeter, indicating the accurate patient positioning on the MR-sim (Fig. 1). No observable positional deviation between registered MR/CT images due to MRI geometric distortion was found. The center position difference of the intra-observer contoured GTVs was -0.05±0.21mm (mean±SD), 0.03+0.20mm, -0.01±0.24mm and 0.33±0.19mm in LR, AP, SI and 3D, respectively. The distributions of the intra-observer lesion positional difference between two delineations were all smaller than 1mm, i.e. the voxel size, as shown in Fig. 2. The contoured lesion volumes (1.91±5.86 cc v.s. 1.90±5.78 cc) showed excellent delineation consistency (intraclass correlation coefficient ICC=0.999) and insignificant intra-observer difference (p=0.367, paired t-test). The DSC between two delineations was 0.85±0.10 (range: 0.49-0.97), indicating excellent intra-observer delineation agreement even in most very small lesions. Only two lesions with the delineation-averaged volume of 0.07cc and 0.02cc were associated with the DSC smaller than 0.5, others were all greater than 0.70. The DSC showed a trend to increase with BM volume as depicted in Fig. 3. The average Hausdorff distances were 0.27±0.17 mm (range: 0.06-1.04mm). also indicating the excellent delineation consistency and reliability.DISCUSSION
It has been established that the response of BM to SRS is better for smaller lesions (3). As such, sensitive CE-T1-SPACE that has high detectability of very small BM should benefit early aggressive SRS treatment and thus patient outcome (4). The patient positioning was accurate on the 1.5T MR-simulator in the exact treatment position and thus met the critical accuracy requirement of SRS. In addition to superior detectability, the highly consistent target delineation based on CE-T1-SPACE was also valuable in SRS treatment planning to guarantee the precise radiation delivery to the exact position of the targets with high dose conformity. On the other hand, this study had limitations and should be further strengthened by increasing patient sample size, including inter-observer disagreement analysis and radiation dose effect evaluation.CONCLUSION
CE-T1-SPACE on a 1.5T MR-simulator facilitated high patient positioning accuracy, superior BM detectability and reliable GTV delineation, so should be of great value in the treatment planning of BM SRS and thus potentially benefits treatment outcome.Acknowledgements
No acknowledgement found.References
1. Suh JH. Stereotactic radiosurgery for the management of brain metastases. N Engl J Med 2010;362(12):1119-1127.
2. Kato Y, Higano S, Tamura H, et al. Usefulness of contrast-enhanced T1-weighted sampling perfection with application-optimized contrasts by using different flip angle evolutions in detection of small brain metastasis at 3T MR imaging: comparison with magnetization-prepared rapid acquisition of gradient echo imaging. AJNR Am J Neuroradiol 2009;30(5):923-929.
3. Chang EL, Hassenbusch SJ, 3rd, Shiu AS, et al. The role of tumor size in the radiosurgical management of patients with ambiguous brain metastases. Neurosurgery 2003;53(2):272-280.
4. El Shafie RA, Paul A, Bernhardt D, et al. Robotic Radiosurgery for Brain Metastases Diagnosed With Either SPACE or MPRAGE Sequence (CYBER-SPACE)-A Single-Center Prospective Randomized Trial. in press, Neurosurgery 2018.
Figures