2375
MRI-based radiomic to predict lipomatous soft tissue tumors malignancy1CREATIS CNRS UMR 5220; Inserm U1206; INSA-Lyon; UCBL Lyon 1, Université de Lyon, Villeurbanne, France, 2Department of Radiology, Centre de lutte contre le cancer Léon Berard, Lyon, France, 3Department of Oncology, Centre de lutte contre le cancer Léon Berard, Lyon, France, 4CREATIS CNRS UMR 5220; Inserm U1206; INSA-Lyon; UCBL Lyon 1, Université de Lyon, Lyon, France
Synopsis
In this study a MRI-based radiomic method was developed to predict lipomatous soft tissue tumors malignancy. 81 subjects with lipomatous soft tissue tumors whose histology was known and with fat-suppressed T1w contrast enhanced MR images available were retrospectively enrolled to constitute a database. A linear support vector machine was used after learning base dimension reduction to develop the model. Results demonstrate that the evaluation of lipomatous tumor malignancy is feasible with good diagnosis performances using a routinely used MRI acquisition in clinical practice.
Introduction
Lipomatous soft tissue tumors can be either benign (such as lipomas) or malignant (liposarcomas) (1,2). The diagnosis between benign lipoma and malignant lipomatous soft tissue tumors is crucial since it directly drive the therapy strategy. Histology is the gold standard for the diagnosis. Nevertheless, due to the invasive aspect of biopsy and its cost, there is a medical need in non-invasive methods to limit the number of unnecessary biopsy. This challenge can be addressed using medical imaging, which is used in routine clinical practice for cancer diagnosis and staging in oncology. However, tumor heterogeneity introduces a wide range of imaging appearance and reduces the performance of conventional imaging features to distinguish between benign and malignant forms of lipomatous tumors. The difficulty is particularly located between lipomas and well-differentiated liposarcomas (WDL) or atypical lipomatous tumors (ALT). It has been reported that MRI has a positive predictive value of 47% in the diagnosis of ALT/WDL because of morphological overlap with many benign lipoma variants [3]. Therefore, many biopsies done for benign lesions could be avoided and more specific methods are needed. The goal of this study is to develop and validate a MRI-based radiomic method to predict soft tissue tumors malignancy.Methods
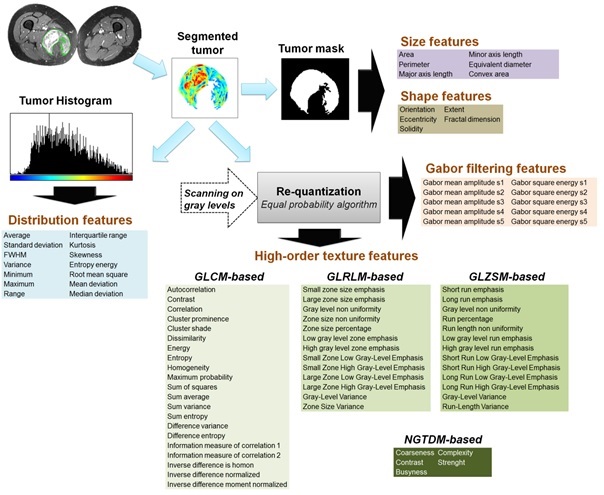
81 subjects with lipomatous soft tissue tumors with histology and contrast-enhanced T1w MR images available were retrospectively enrolled. Repartition according to tumor histology was n = 40 lipomas and n = 41 WLD/ALT. MR images were obtained from 56 different centers with non-uniform protocols. Acquisitions were performed at 3 different fields (1.0T, 1.5T, and 3.0T) with 18 different MR systems commercialized by 4 vendors. In 65% of cases, images were acquired with a 2D fast spin echo sequence (53.3% with a fat saturation and 11.7% with a fat-water decomposition); in 4.9% of cases with a 3D isotropic fast spin echo sequence and in 35% of cases with a 3D gradient echo sequence (16.5% with a fat saturation and 13.6% with a fat-water decomposition). Mean pixel size was 0.81² ± 0.29² mm² (range: 0.37² – 1.75² mm²). Images were automatically loaded on an in-house software developed on Matlab R2017a. The tumor was segmented manually by two observers to evaluate the inter-observer reproducibility. Tumor mask was next applied on fat-suppressed enhanced MR image and 87 radiomic features were extracted. They included size, shape, intensity distribution, image domain (based on GCLM, GLRLM, GLSZM and NGTDM matrices) and frequency domain (based on Gabor filtering) textures features. (Fig.1) The set of initial features was reduced to decrease the risk of overfitting and create another set of relevant features in term of relevancy and inter-observer reproducibility. This procedure was achieved using a backward selection by a double thresholding on t-test p-value (t < 0.1) and Pearson’s correlation coefficient (t > 0.8), beforehand computed in the reproducibility study. Next, a classification model was built from a support vector machine with a linear kernel. Before training, data were centered at their mean and scales to have unit standard deviation. Support vector computation and hyperplane separation was done using a sequential minimal optimization. Internal validation was performed using a holdout cross-validation method (75% of data were used for training and 25% for test).Results
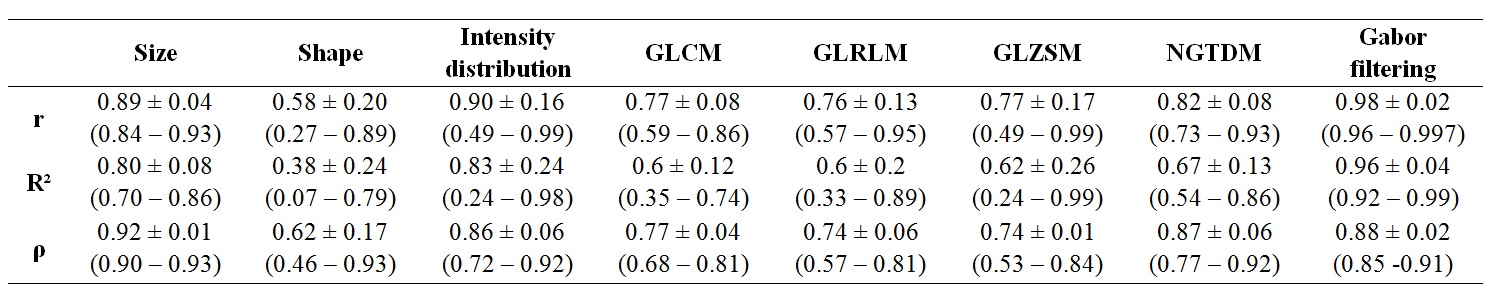
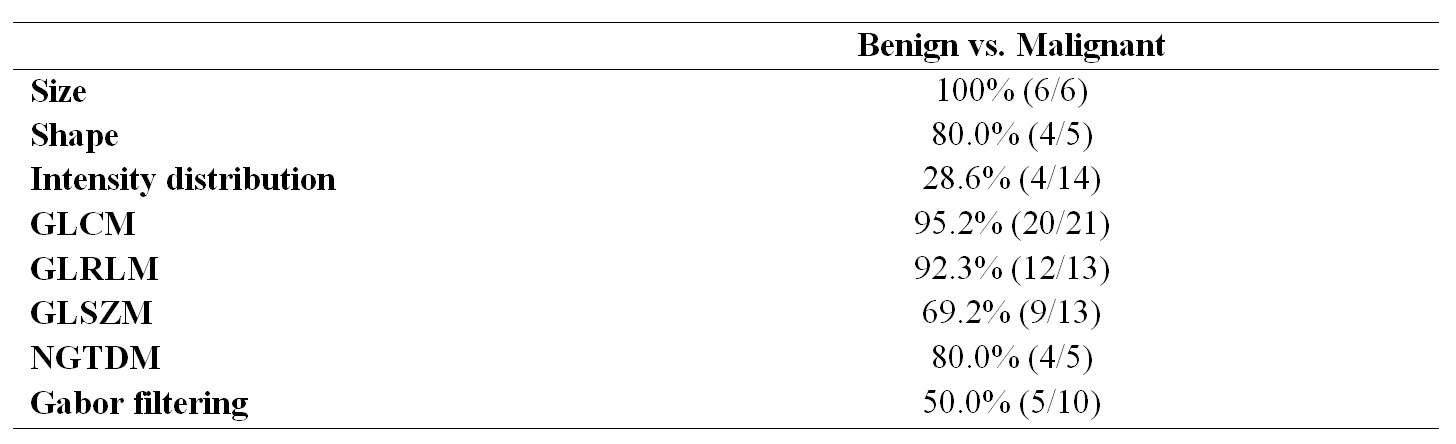
For the whole set of radiomic features, Pearson’s correlation coefficient was ranged between 0.27 and 0.99; mean: 0.81 ± 0.15. Based on a 0.8 threshold on the Pearson’s correlation coefficient, 63.2% of radiomic features (55/87) were considered reproducible. Results for all features families are summarized in Fig.2. Based on t-test p-value, 73.6% of features (64/87) were found relevant to be included in the reduced feature set. Results stratified by feature family are summarized in Fig.3. After combination with reproducibility criterion, the radiome was finally reduced to 35 features (40.2%). To predict malignant tumors, model diagnosis performances were: AUROC = 0.96; sensitivity = 100% (95% CI: 100 – 100%); specificity = 90% (95% CI: 71.4 – 108%); positive predictive value = 90.9% (95% CI: 73.9 – 108%); negative predictive value = 100% (95% CI: 100 – 100%) and overall accuracy = 95.0% (95% CI: 85.5 – 105%).Discussion
These results show that the evaluation of lipomatous tumor malignancy is feasible using a routinely used MRI acquisition in clinical practice. As suggested by the reproducibility study, the segmentation step may introduce inherent inter-observer variability and this latter need to be taking into account in the data mining. These encouraging results need to be further confirmed on an external validation cohort.Acknowledgements
This work was performed within the framework of the SIRIC LyriCAN grant INCa_INSERM_DGOS_12563 and LABEX PRIMES (ANR-11-LABX-0063), program "Investissements d'Avenir" (ANR-11-IDEX-0007).References
(1) Murphey M et al. Radiographics 2005; 25:1371-1395.
(2) O’Regan et al. Am J Roentgenol 2011; 97:37-43.
(3) Brisson M et al. Skelet Radiol 2013; 42:635-647.
Figures