2363
Characterising early stage cervical cancer using radiomic features derived from T2- and diffusion-weighted images: a potential prognostic tool in surgical management?1Cancer Research UK Imaging Centre, The Institute of Cancer Research, Sutton, United Kingdom, 2MRI Unit, The Royal Marsden Hospital NHS Foundation Trust, Sutton, United Kingdom, 3Gynaecology Unit, The Royal Marsden Hospital NHS Foundation Trust, London, United Kingdom, 4Gynaecology, St. Georges University Hospital, London, United Kingdom
Synopsis
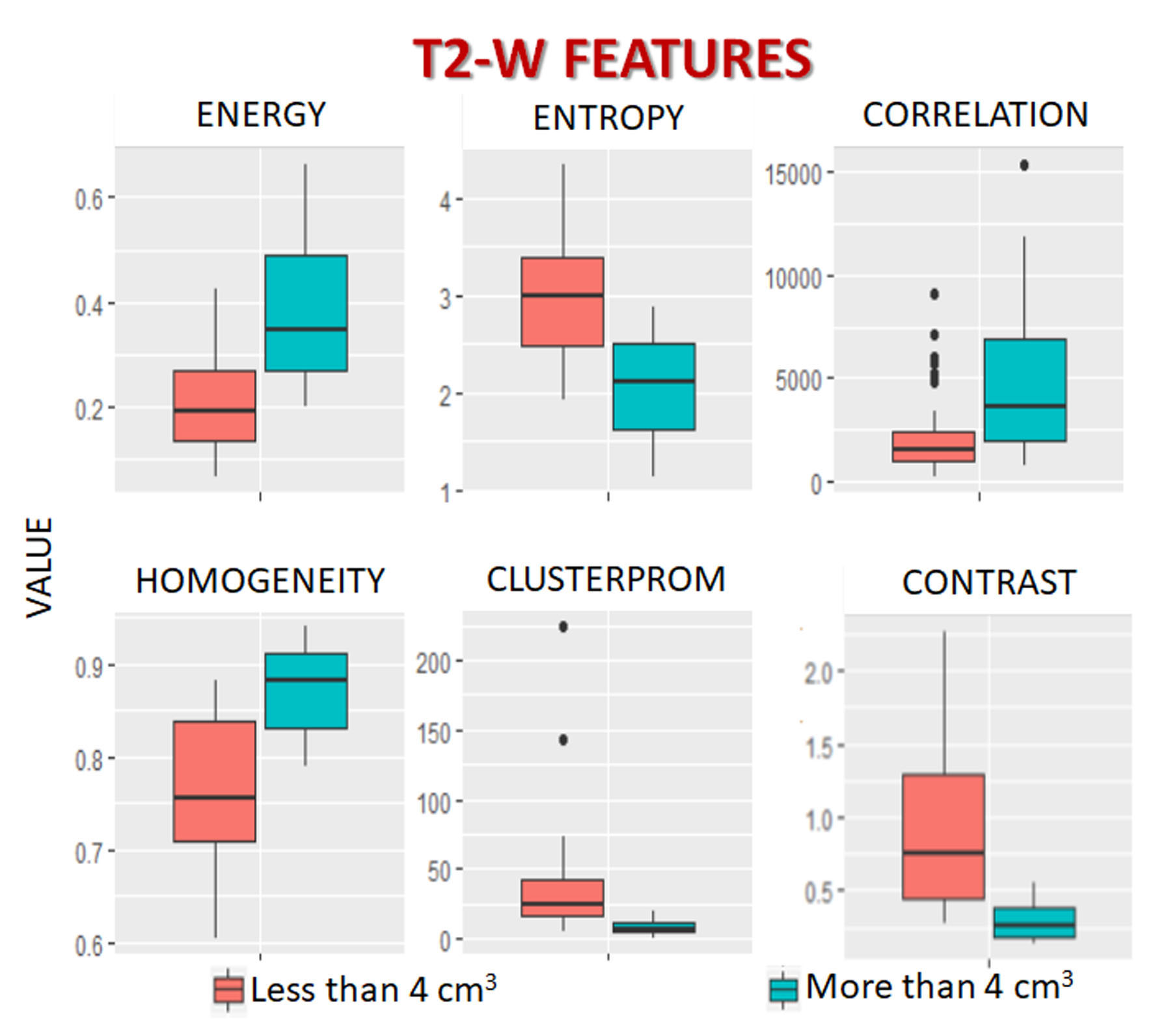
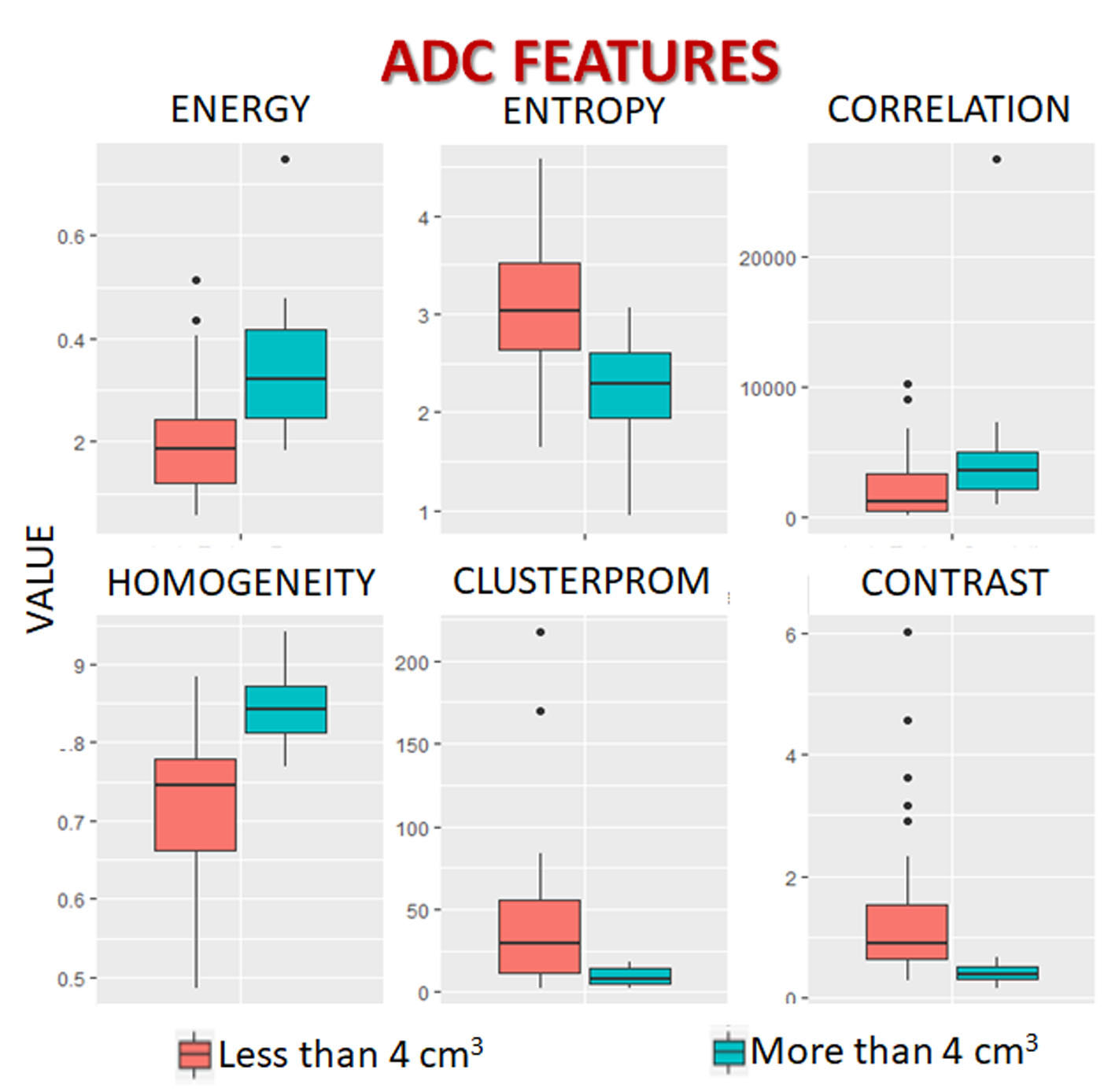
Radiomic features were compared between cervical tumors below and above the volume threshold of eligibility for trachelectomy (< or >4 cm3) to determine their potential prognostic value. Textural feature differences between smaller and larger tumors were similar for both the T2-W and the ADC data. Homogeneity and Energy were increased and Entropy, Contrast and Cluster Prominence decreased in larger tumors. This may reflect the transition from a mixed morphology (tumor elements interspersed with normal glands and stroma) in smaller tumors to more homogenous sheets of malignant cells as tumors increase in size and de-differentiate.
Introduction
Stage 1 cervical cancer is treated surgically. The extent of surgery (cone biopsy, radical trachelectomy or hysterectomy) depends on tumor resectability and risk of recurrence and is influenced by the patients’ desire to retain fertility. Resectability is largely determined by pre-operative tumor volume, which is a powerful adverse prognostic factor1. Other prognostic factors influence choice of surgical management and are derived from biopsy (tumor type, grade, lymphovascular space invasion and depth of stromal invasion2, so may not represent the tumor in its entirety. In these cases, pre-operative imaging features of adverse outcome would enable selection of the optimal surgical technique.
It is possible to convert imaging data into a high-dimensional mineable feature space (radiomics). Radiomic features may be extracted from T2-W3 as well as diffusion-weighted data4, both of which are routinely used for identifying cervix cancer. As radiomic output is crucially affected by image noise, (a problem in diffusion-weighted data and when the lesion of interest is small), data can be acquired using an endovaginal receiver coil to maximize signal-to-noise ratio from the cervical tumor5.
Aim
To identify radiomic features that were significantly different between cervical tumors that are below and above the volume threshold of eligibility for trachelectomy (less or greater than 4 cm3, equivalent to a spherical volume of ~2 cm diameter) in order to determine their potential prognostic value.Methods
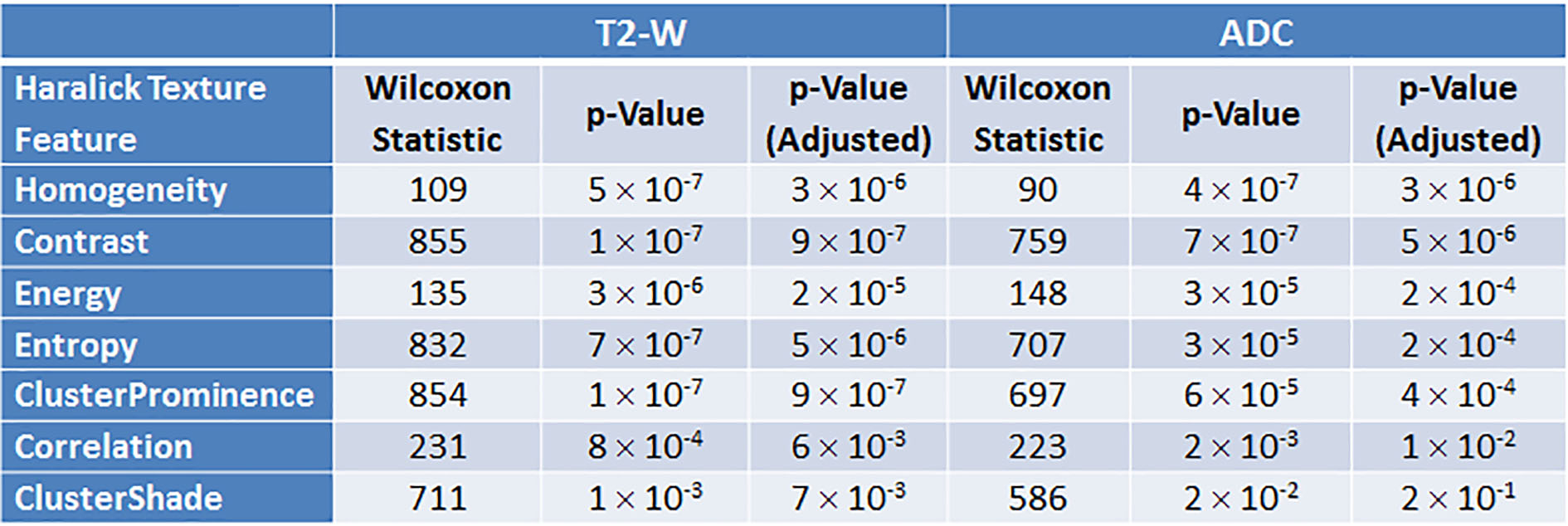
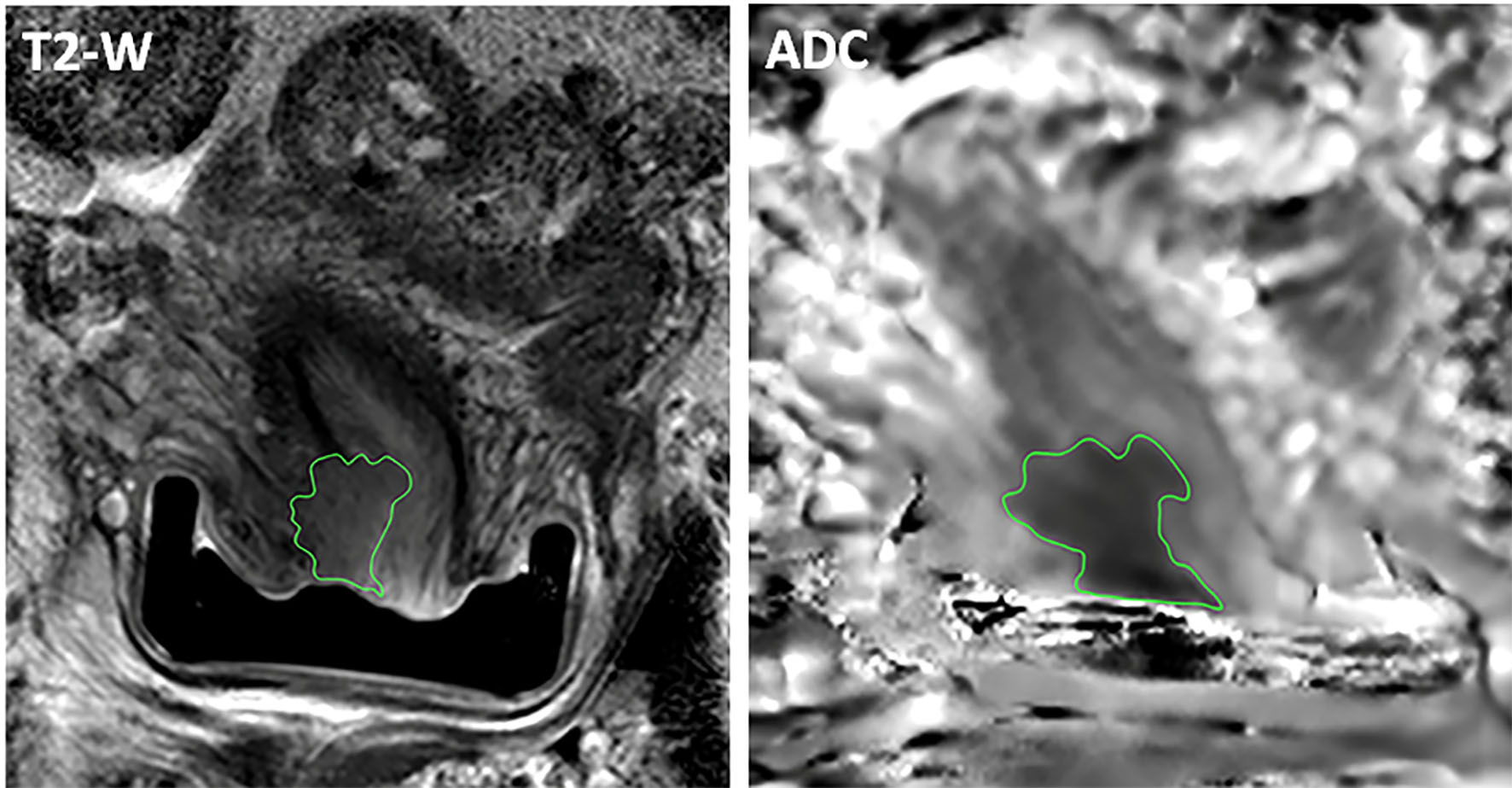
We identified patients (n=61, aged 24-77 years, mean 36.9 ± 12.1 years) who had undergone endovaginal MRI for cervical cancer between March 2014 and October 2017 as part of an on-going IRB approved research study and given written consent for use of their data were identified. Inclusion criteria imposed a tumor volume of 0.2 cm3 as minimum6,7 with artefact-free images. Scans were anonymized and, using OsiriX software (Pixmeo SARL, Bernex, Switzerland), 2-D regions-of-interest (ROI) were drawn around the whole tumor by an experienced (25 years) observer on each slice demonstrating tumor. The contour data for all the separate 2-D ROIs were aggregated and exported to our image data platform XNAT8 as a single DICOM RT-STRUCT file, corresponding to a 3-D tumour volume. Custom in-house software was used to extract textural features from the MRI images using Haralick texture analysis9. These features are computed from the Grey Level Co-occurrence Matrices (GLCM) at each voxel underlying the ROI in a 3D volume. Correlated Haralick features were eliminated prior to analysis leaving seven features for interrogation by volume10. These were Homogeneity, Contrast, Energy, Entropy, Cluster prominence, Correlation and Cluster shade. A Wilcoxon rank sum test with Bonferroni correction was applied to assess the differences in these features between tumors less than or greater than 4 cm3.Results
Of 61 patients, 39 had a tumor volume < 4 cm3 (range 0.3 – 3.6 cm3, mean 1.0 ± 1.1 cm3) and 22 had a tumor volume >4 cm3 (range 4.2-56.1 cm3, mean 15.1 ± 12.6 cm3) (Figure 1). After Bonferroni correction, 6 of 7 texture features on both T2-W and ADC remained significant, namely Homogeneity, Contrast, Energy, Entropy, Cluster prominence and Correlation (Table 1, Figure 2).Discussion and Conclusions
The pattern of radiomic differences between tumors less than or greater than 4 cm3 were similar for both the T2-W and the ADC data. There was a greater tendency to increased Homogeneity in larger tumors, indicating that grey levels in adjacent pixels were similar in larger tumors. This was borne out by the reduction in Contrast which was lower in larger tumors. Energy, which is a measure of textural uniformity and is highest when grey level distribution has either a constant or a periodic form was also higher in larger tumors. Entropy measures the disorder of an image; when the image is not texturally uniform many GLCM elements have very small values, so that entropy is inversely proportional to GLCM energy. Entropy was higher in smaller tumors indicating their non-uniformity both on the T2-W imaging and ADC maps. This initial data indicates for the first time using radiomic analysis, that as cervical tumors grow, they tend to become texturally more homogenous. This may well reflect the transition from a morphology where tumor elements are interspersed with normal cervical glandular elements and stroma in smaller tumors to more homogenous sheets of malignant cells as tumors increase in size and de-differentiate. Correlation of radiomic with histological features will be needed to validate these findings.Acknowledgements
CRUK support to the Cancer Imaging Centre at ICR and RMH in association with MRC and Department of Health C1060/A10334, C1060/A16464 and NHS funding to the NIHR Biomedical Research Centre and the Clinical Research Facility in Imaging.References
- Alfsen GC, Kristensen GB, Skovlund E et al. Histologic subtype has minor importance for overall survival in patients with adenocarcinoma of the uterine cervix: a population-based study of prognostic factors in 505 patients with nonsquamous cell carcinomas of the cervix. Cancer. 2001; 92: 2471-83.
- Halle MK, Ojesina AI, Engerud H, et al. Clinicopathologic and molecular markers in cervical carcinoma: a prospective cohort study. Am J Obstet Gynecol. 2017; 217: 432.e1-432.e17.
- Hou Z, Li S, Ren W, et al. Radiomic analysis in T2W and SPAIR T2W MRI: predict treatment response to chemoradiotherapy in esophageal squamous cell carcinoma. J. Thorac. Dis. 2018; 10: 2256-2267.
- Wang Q, Li Q, Mi R, et al. Radiomics Nomogram Building From Multiparametric MRI to Predict Grade in Patients With Glioma: A Cohort Study. J Magn Reson Imaging. 2018.
- Gilderdale DJ, deSouza NM, Coutts GA, et al. Design and use of internal receiver coils for magnetic resonance imaging. Br J Radiol. 1999; 72(864):1141-51.
- Charles-Edwards EM, Messiou C, Morgan VA, et al. Diffusion-weighted imaging in cervical cancer with an endovaginal technique: potential value for improving tumor detection in stage Ia and Ib1 disease. Radiology. 2008; 249: 541-50.
- deSouza NM, Dina R, McIndoe GA, Soutter WP. Cervical cancer: value of an endovaginal coil magnetic resonance imaging technique in detecting small volume disease and assessing parametrial extension. Gynecol Oncol. 2006; 102: 80-5.
- Marcus, DS, Olsen, TR, Ramaratnam, M and Buckner, RL. The extensible neuroimaging archive toolkit. Neuroinformatics 2007; 5: 11-33.
- Haralick, RM and Shanmugam, K. Textural features for image classification. IEEE Trans. Systems, Man, and Cybernetics; 6: 610-621.
- Wibmer, A., Hricak, H.,
Gondo, T. et al. Haralick texture analysis of
prostate MRI: utility for differentiating non-cancerous prostate from prostate
cancer and differentiating prostate cancers with different Gleason scores. Eur Radiol. 2015;
25: 2840.
Figures