2359
Readout-segmented vs. Single Shot Diffusion MRI for Radiation Therapy Planning in Head and Neck Tumor1Dept.of Radiology, Medical Physics, Medical Center University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany, 2German Cancer Consortium (DKTK), Partner Site Freiburg, Freiburg, Germany, 3Department of Radiation Oncology, Medical Center University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany
Synopsis
Image distortion is a major limitation in radiation therapy (RT) planning, especially for diffusion weighed imaging in regions with strong B0-inhomogeneity. In this study we analyze the improvement of Readout-segmented-EPI over conventional single shot EPI in the geometrically challenging anatomical region of the neck. RS-EPI effectively increases geometric accuracy in head and neck tumor DWI and significantly reduces ghosting artifacts at the cost of a slightly prolonged acquisition time. Therefore it has proven a clear clinical benefit compared to standard SS-EPI.
Introduction
Image distortion is a major limitation in radiation therapy (RT) planning, in particular, if gross tumor volumes (GTVs) are defined in multi-parametric MRI data. Diffusion weighted imaging (DWI) in particular has been shown to be a good discriminator between tumor and normal tissue, and is thus a standard method in various cancer protocols, e.g. PI-RADS1 or BI-RADS2,3.
However, DWI is typically performed with single shot EPI which is highly sensitive to B0-field inhomogeneities that can cause severe geometrical distortions. Distortions can be reduced by increasing the effective bandwidth in phase encoding direction with acceleration techniques such as GRAPPA or SENSE, partial Fourier acquisition or by the use of non-EPI methods as SNAILS4, PROPELLER5 or Turboprop6. Another alternative is readout-segmented EPI (RS-EPI)7,8 which has been shown to dramatically decrease image distortions9,10.
In this study we analyze the improvement of RS-EPI over conventional single shot EPI in the geometrically challenging anatomical region of the neck. In a patient study with head&neck tumors we compare the geometrical accuracy, influence of image artifacts as well as physical plausibility of the measured apparent diffusion coefficient (ADC) maps.
Materials and Methods
In a prospective RT study in head and neck tumors, a total of 25 patients were imaged at a 3 T MRI system (TIM Trio, Siemens, Erlangen, Germany) including conventional EPI and RS-EPI in week 0 (before treatment) and 2 and 5 weeks into RT. After excluding missing and corrupted data, 44 cases with conventional EPI and 51 cases with RS-EPI were considered.
In this study, we used a single shot diffusion weighted EPI sequence with sequence parameters: TE = 71 ms, TR = 3500 ms, reconstructed resolution = 2×2×3 mm3. The readout-segmented sequence used TE = 51 ms, TR = 2510 ms, reconstructed resolution = 2×2×3 mm3 with 7 shots per image. Both sequences used 3 diffusion weightings with b = {50,400,800} s/mm2. Considering parallel imaging and partial Fourier methods, the bandwidth per pixel BWPx amounted to 19.5 Hz/px for conventional EPI, and 48.8 Hz/px for the RS-EPI. The geometric distortion Δx is dependent on the B0-field inhomogeneity ΔB0 and BWPx in phase encoding direction $$$Δx = γ ΔB_0 / BW_{Px}$$$.
To validate that the geometric distortions are solely caused by B0 off-resonances, a field map was measured in a volunteer together with the DWI sequences. In the patient study, In the gross tumor volume and the volume of the lymph node metastasis (GTV-T and GTV-LN), additionally, ADC values were compared between EPI and RS-EPI.
Results
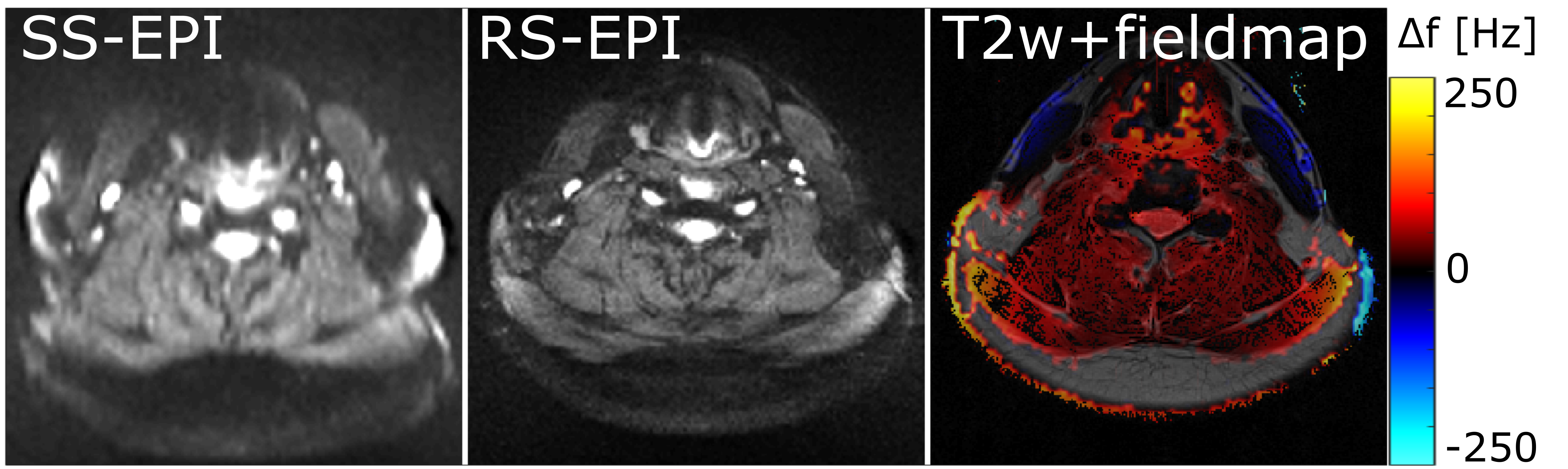
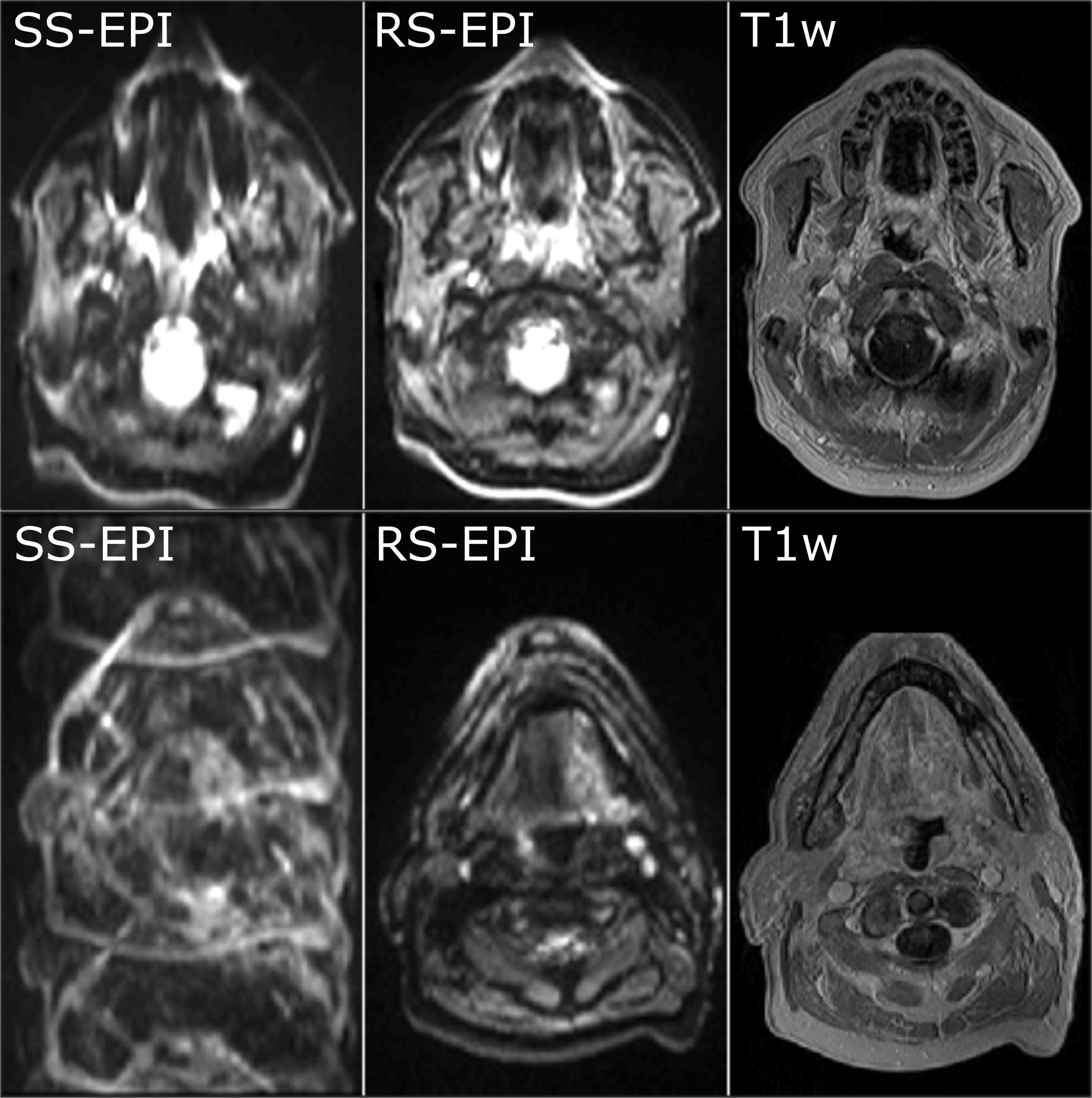
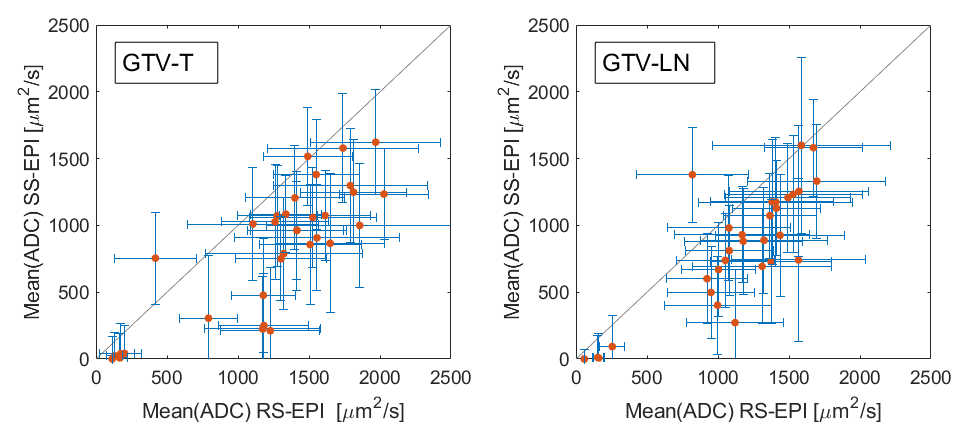
In the volunteer, off-resonances up to ±250 Hz were found causing shifts of up to 13px/5px for EPI/RS-EPI (Fig.1). The geometric distortion does not only include stretch or shear of the whole image, but also locally fast oscillating changes, as shown in Fig.2. With increasing off-resonance, ghosting artifacts become visible. For conventional EPI, only 5% of the images were completely artifact-free, whereas 75% of the RS-EPI measurements did not show the artifact. Figure 2 shows an example of conventional EPI with a 4-fold ghost artifact and a RS-EPI without apparent artifacts. Additionally, frequency-selective fat suppression was challenging for both sequences due to the field inhomogeneity. Figure 3 shows the mean ADC values for conventional and RS-EPI in GTV-T and GTV-LN in a scatter plot. Conventional EPI yields systematically smaller ADC values than RS-EPI for both cases, while their individual standard deviations do not differ.Discussion
The neck region is especially challenging for single shot EPI as the magnetic field inhomogeneities from the complex anatomy cannot be corrected by a second order shim. Strong off-resonances lead to ghosting artifacts which mask diagnostically relevant areas. Ghosting also affects the ADC-maps, as signal is leaking into other parts of the image effectively decreasing SNR in the GTVs. As DWI is an inherently low-SNR technique for high b-values, this SNR decrease can lead to systematic errors in the ADC calculation11. If the artifact leads to signal overlap from different anatomical regions, the resulting ADC will also show a mixture of the two regions.
Recently, field inhomogeneities in the neck region were partially compensated using a dielectric pillow12; however, these pillows are impractical in a patient study, as the additional weight is often not tolerated by the patient. Alternatively, locally integrated shim coils might be used to increase field homogeneity13.
RS-EPI effectively increases geometric accuracy in head and neck tumor DWI and significantly reduces ghosting artifacts at the cost of a slightly prolonged acquisition time. In line with studies in the head9,14 or liver15, RS-EPI has proven a clear clinical benefit compared to standard SS-EPI.
Acknowledgements
This work was supported in parts by a grant from the Deutsche Forschungsgemeinschaft (DFG) under grant number HA 7006/1-1.References
1. Steiger P, Thoeny HC. Prostate MRI based on PI-RADS version 2: how we review and report. Cancer Imaging 2016;16:9 doi: 10.1186/s40644-016-0068-2.
2. Yabuuchi H, Matsuo Y, Okafuji T, et al. Enhanced mass on contrast-enhanced breast MR imaging: Lesion characterization using combination of dynamic contrast-enhanced and diffusion-weighted MR images. J. Magn. Reson. Imaging 2008;28:1157–1165 doi: 10.1002/jmri.21570.
3. Burnside ES, Sickles EA, Bassett LW, et al. The ACR BI-RADS® Experience: Learning From History. J. Am. Coll. Radiol. 2009;6:851–860 doi: 10.1016/j.jacr.2009.07.023.
4. Liu C, Bammer R, Kim D, Moseley ME. Self-navigated interleaved spiral (SNAILS): Application to high-resolution diffusion tensor imaging. Magn. Reson. Med. 2004;52:1388–1396 doi: 10.1002/mrm.20288.
5. Pipe JG, Farthing VG, Forbes KP. Multishot diffusion-weighted FSE using PROPELLER MRI. Magn. Reson. Med. 2002;47:42–52 doi: 10.1002/mrm.10014.
6. Pipe JG, Zwart N. Turboprop: Improved PROPELLER imaging. Magn. Reson. Med. 2006;55:380–385 doi: 10.1002/mrm.20768.
7. Porter DA, Heidemann RM. High resolution diffusion-weighted imaging using readout-segmented echo-planar imaging, parallel imaging and a two-dimensional navigator-based reacquisition. Magn. Reson. Med. 2009;62:468–475 doi: 10.1002/mrm.22024.
8. Holdsworth SJ, Skare S, Newbould RD, Guzmann R, Blevins NH, Bammer R. Readout-Segmented EPI for Rapid High Resolution Diffusion Imaging at 3T. Eur. J. Radiol. 2008;65:36–46 doi: 10.1016/j.ejrad.2007.09.016.
9. Zhao M, Liu Z, Sha Y, et al. Readout-segmented echo-planar imaging in the evaluation of sinonasal lesions: A comprehensive comparison of image quality in single-shot echo-planar imaging. Magn. Reson. Imaging 2016;34:166–172 doi: 10.1016/j.mri.2015.10.010.
10. Tullos H, Dale B, Bidwell G, et al. SU‐E‐I‐67: Multi‐Shot RESOLVE Compared to Single‐Shot EPI Diffusion‐ Weighted MR Imaging Acquisition Scheme. Med. Phys. 2012;39:3640–3640 doi: 10.1118/1.4734783.
11. Jones DK, Basser PJ. “Squashing peanuts and smashing pumpkins”: How noise distorts diffusion-weighted MR data. Magn. Reson. Med. 2004;52:979–993 doi: 10.1002/mrm.20283.
12. Oudeman J, Coolen BF, Mazzoli V, et al. Diffusion-prepared neurography of the brachial plexus with a large field-of-view at 3T. J. Magn. Reson. Imaging 2016;43:644–654 doi: 10.1002/jmri.25025.
13. Umesh Rudrapatna S, Fluerenbrock F, Nixon TW, de Graaf RA, Juchem C. Combined imaging and shimming with the dynamic multi-coil technique. Magn. Reson. Med. 2018 doi: 10.1002/mrm.27408.
14. Yeom KW, Holdsworth SJ, Van AT, et al. Comparison of readout-segmented echo-planar imaging (EPI) and single-shot EPI in clinical application of diffusion-weighted imaging of the pediatric brain. AJR Am. J. Roentgenol. 2013;200:W437-443 doi: 10.2214/AJR.12.9854.
15. Tokoro H, Fujinaga Y, Ohya A, et al. Usefulness of free-breathing readout-segmented echo-planar imaging (RESOLVE) for detection of malignant liver tumors: Comparison with single-shot echo-planar imaging (SS-EPI). Eur. J. Radiol. 2014;83:1728–1733 doi: 10.1016/j.ejrad.2014.06.013.
Figures