2355
Accuracy and precision of DCE-MRI acquired with golden-angle radial k-space under-sampling1Radiology, Mayo Clinic, Rochester, MN, United States, 2National Centre for Advanced Medical Imaging (CAMI), St James Hospital / Trinity College University of Dublin, Dublin, Ireland, 3Philips Healthcare, Surrey, United Kingdom
Synopsis
The effects of using a continuous golden-angle radial k-space sampling trajectory, with varying degrees of under-sampling and compressed sensing image reconstruction, on the accuracy and precision of pharmacokinetic modeling of DCE data, were quantitatively investigated. DCE image temporal resolutions (Tres) ranging from 1.85s to 0.09s (corresponding to radial sampling densities of 100% to 4.68%) produced absolute accuracy/precision errors in all Ktrans, ve and kep values of ≤ 2%/4% (for Tres =1.85s) to ≤ 12%/11% (for Tres =0.09s), respectively. These results demonstrate that DCE image acquisition protocols can be designed which constrain pharmacokinetic parameter value errors within prescribed thresholds.
Introduction
While an optimum temporal resolution (Tres) for dynamic contrast-enhanced (DCE) MRI remains elusive, it is clear that the accurate measurement of fast-changing contrast time-intensity curve (CTC) shapes in DCE requires short Tres values, particularly for measurements of patient-specific arterial input function (AIF) used in pharmacokinetic (PK) modelling on the data [1]. Compressed sensing (CS) techniques are highly suited to DCE acquisitions, given the inherent sparsity in the temporal domain, and thus they present an ideal solution to reducing Tres values. However, to date no studies have investigated quantitatively the effect that (vastly) undersampling the data has on the fidelity of measuring rapidly changing CTC shapes, and hence on the consequent PK modelling outputs. Quantification of any effect requires a priori knowledge of the ground truth CTC curve shapes, which are never known in vivo. A recent study [2] described a novel phantom design wherein ground truth values were unambiguously known prior to MRI scanning, allowing for direct comparisons between the known ground truth CTCs and those measured on the scanner. In this way, absolute errors as a function of acquisition parameters could be determined. The aim of this study was to quantify the accuracy and precision of DCE-MRI measurements as a function of under-sampling ratio, for data acquired using a continuous golden-angle radial k-space sampling trajectory using the model phantom system.
Methods
A physiologically-relevant AIF curve-shape was extracted from 32 prostate-patient datasets acquired with Tres=3.1s and voxel size=1x1x6mm3. Ground truth CTCs and AIF curve-shapes were subsequently established at the phantom using a highly-precise optical imaging, with repeatability of the phantom evaluated via 10 repeat measurements[2]. DCE-MRI data were acquired of the phantom using a 3T scanner (Achieva; Philips, Netherlands) and a 32-channel detector coil. A multi-slice 2D turbo-field-echo FFE (SPGR) sequence was employed, with a stack-of-stars golden-angle radial trajectory and 97,200 (32,400 per slice) radial spokes acquired continuously with a total acquisition duration of 470s (TR/TE=10.5/1.6ms, α=38°, FOV=224x224x18mm3, voxels=1.75x1.75x6mm3). Each experiment consisted of two measurements of the AIF and either the ‘tumor’ or ‘healthy’ CTC, each repeated on 5 separate days, and 5-times within the same session. B1+ maps were acquired using a dual-steady-state sequence with the same geometry and spatial resolution (TR1/TR2/TE=30ms/150ms/2ms, α=60°), and were used to correct for B1+-field non-uniformities. All calibration and CS image reconstruction [3] was performed using the BART toolbox [4], at radial sampling densities ranging from 100%-4.68%, giving a Tres range from 1.85-0.09s. Root mean square errors (RMSE) and concordance correlation coefficient (CCC) values were calculated between the MR-measured and ground truth AIFs. Pharmacokinetic (PK) modeling was performed using a linear version of the standard Tofts model, with resultant Ktrans, ve and kep values compared against the known ground truth values.Results
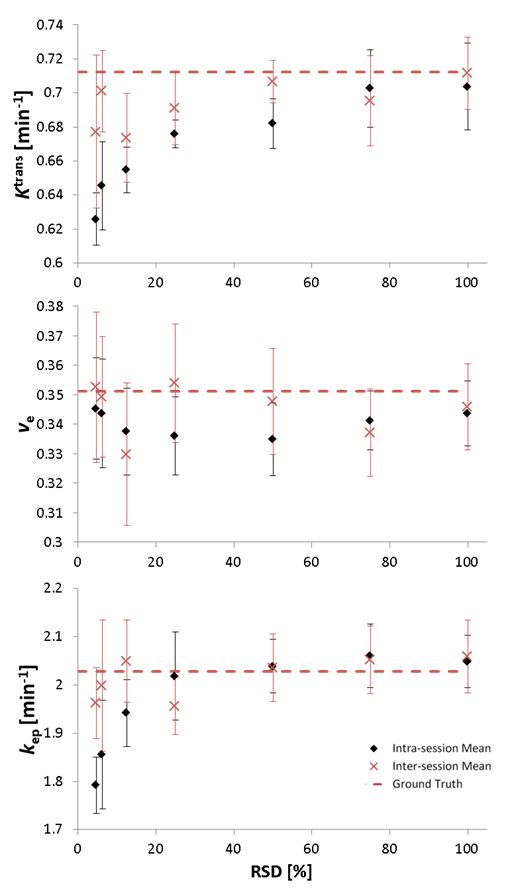
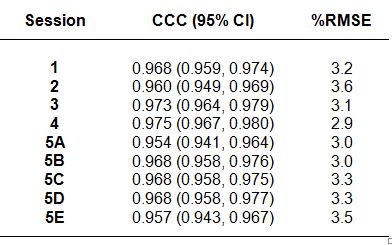
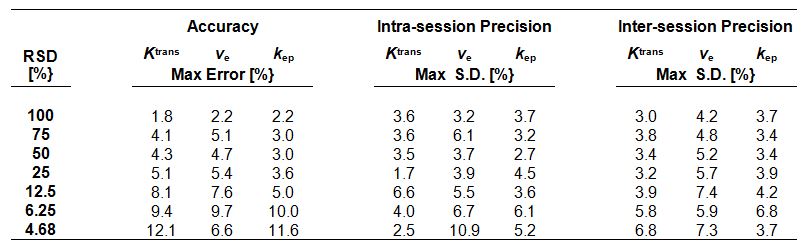
The 10 repeat phantom measurements had CCC>0.995, RSME≤1% (translates to a variation in PK parameter value outputs of ±0.3-0.8%). CCC values (Table 1) in the range [0.95-0.98] were measured across intra-/inter-session acquisitions, demonstrating a high degree of precision for the measured CTC curve shapes. Corresponding RSME values were in the range [2.9%-3.6%]. Images reconstructed at RSD=100% produced PK parameters (Ktrans, ve and kep) with errors all less than 2% and intra-/inter-session standard deviations all less than 4%. Both accuracy and precision reduced with reduced RSD; however, even at the lowest RSD tested (RSD=4.68%) all PK parameters were calculated with errors ≤12%, intra-session standard deviation ≤11%, and inter-session standard deviation ≤7%.Discussion
The accuracy and precision that is required for PK parameter values derived from DCE-MRI image data is not known, and is ultimately dependent upon the differences in PK parameter values one expects to measure clinically in, say, a tumor versus healthy tissue, or in assessing longitudinally changes in a tumor during therapy. This uncertainty is fuelled largely by the lack of standardization of DCE acquisition protocols and consequent very broad range of published PK parameter values for tumors. The data presented herein provides DCE acquisition parameters for a rapidly-accelerated radial sequence which can be used to constrain errors within known values, while the continuous golden-angle radial acquisition approach facilitates greater flexibility with regards to choosing the desired/required Tres and a lower sensitivity to motion.Conclusions
The effects of undersampling on the accuracy and precision of PK modeling of DCE data has been investigated. Acquisition parameters required to constrain errors within known values were determined. The results presented herein point towards an optimum, validated, fast DCE acquisition and image reconstruction methodology, which may contribute towards a greater standardization of DCE protocols the wider adoption of this technique into the clinical arena.Acknowledgements
Supported by Irish Cancer Society Research Scholarship CRS13KNI and Philips Healthcare Clinical Science.References
1] Henderson E, Rutt BK, Lee TY. Temporal sampling requirements for the tracer kinetics modeling of breast disease. Magn Reson Imaging. 1998;16:1057-73.
[2] Knight SP, Browne JE, Meaney JF, Smith DS, Fagan AJ. A novel anthropomorphic flow phantom for the quantitative evaluation of prostate DCE-MRI acquisition techniques. Phys Med Biol. 2016;61:7466-83.
[3] Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn Reson Med. 2007;58:1182-95.
[4] Uecker M, Lai P, Murphy MJ, Virtue P, Elad M, Pauly JM, et al. ESPIRiT — An Eigenvalue Approach to Autocalibrating Parallel MRI: Where SENSE meets GRAPPA. Magn Reson Med. 2014;71:990-1001.
Figures