2346
MRI Independent Predictors of Pathological Complete Response to Neoadjuvant Chemoradiotherapy in Locally Advanced Rectal Cancer1Department of Diagnostic Radiology, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
Synopsis
In order to tapped the potential of pCR prediction on T2WI comprehensively, both quantitative and qualitative parameters were evaluated in patients with locally advanced rectal cancer. A development group were enrolled to assess these parameters and an external validation group to verify the diagnostic performance. Post-nCRT CATV (CATVpost) and the reduction rate of SIT (SITRR) were proved that were independently associated with pCR and can help for pCR prediction.
Introduction
There has been a gradual shift from radical surgery following neoadjuvant chemoradiotherapy(nCRT) to “wait-and-see” strategy for patients with pathological complete response (pCR) in locally advanced rectal cancer(LARC), however, identifying patients with pCR using a noninvasive test currently is a challenge. This study aim to investigate the effective quantitative and qualitative parameters on T2-weighted magnetic resonance imaging (MRI) for predicting pCR in patients with LARC.
Methods
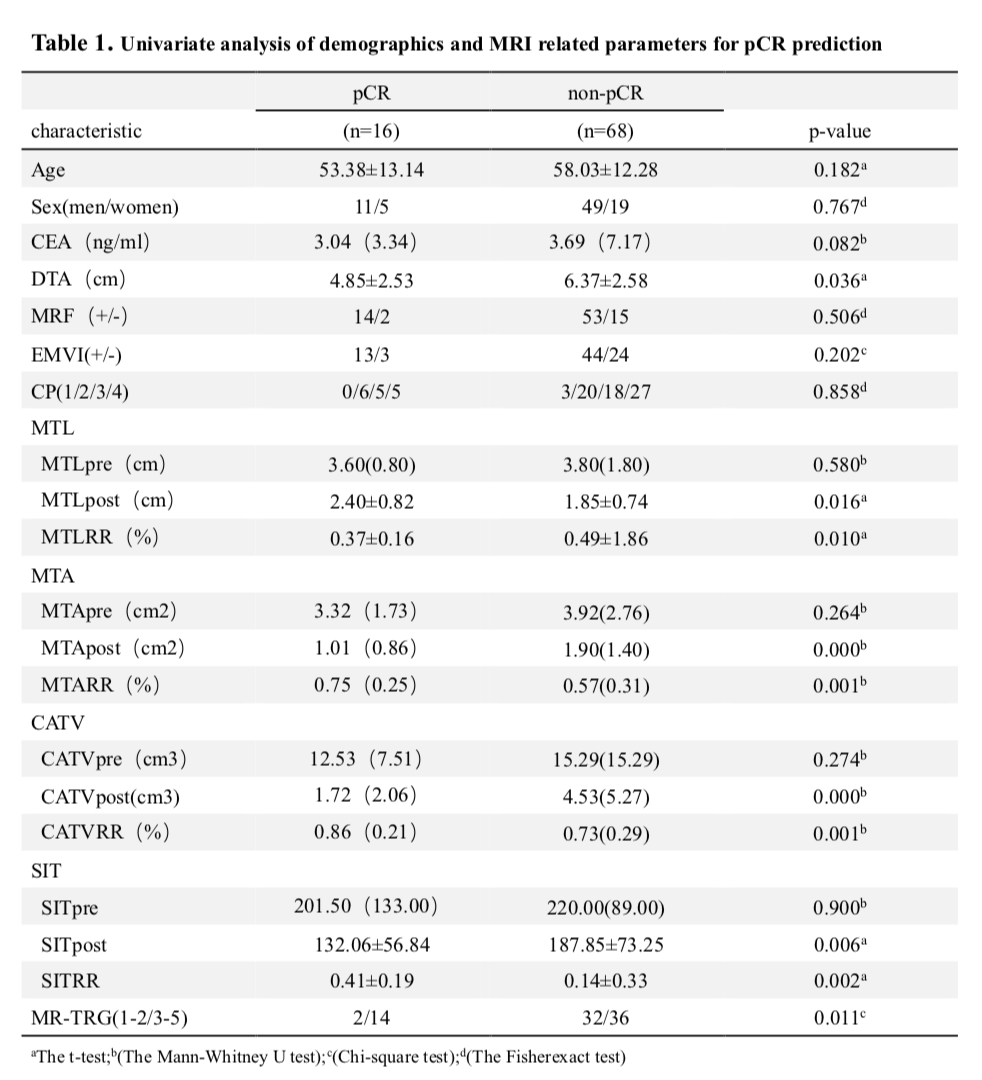
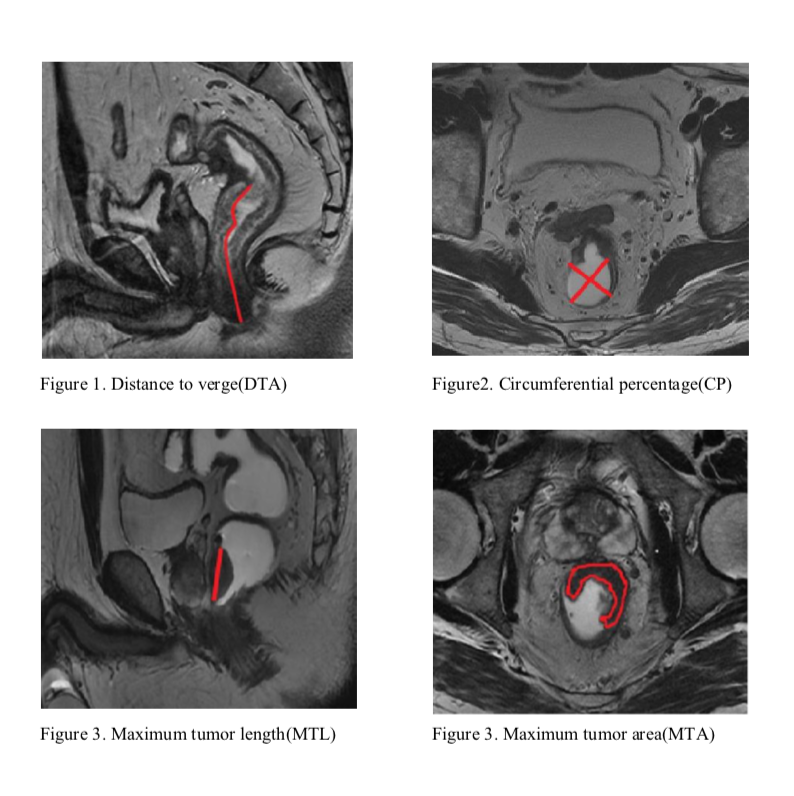
Eighty-four consecutive patients were enrolled who had undergone pre- and post-CRT MRI. Quantitative parameters including maximum tumor length(MTL), maximum tumor area(MTA), cylindrical approximated tumor volume(CATV) and signal intensity (SIT) were measured, the reduction rate of them were calculated, and the tumor regression grade on MRI(MR-TRG) and conventional MRI features also were evaluated. A multivariate logistic regression analysis was performed to analysis the effective parameters for predicting pCR before surgery. An external cohort of 36 patients as a validation group to verify the pCR prediction protocol. And receiver operating characteristic (ROC) analysis was used to assess the diagnostic performance of developmentand validation group.
Results
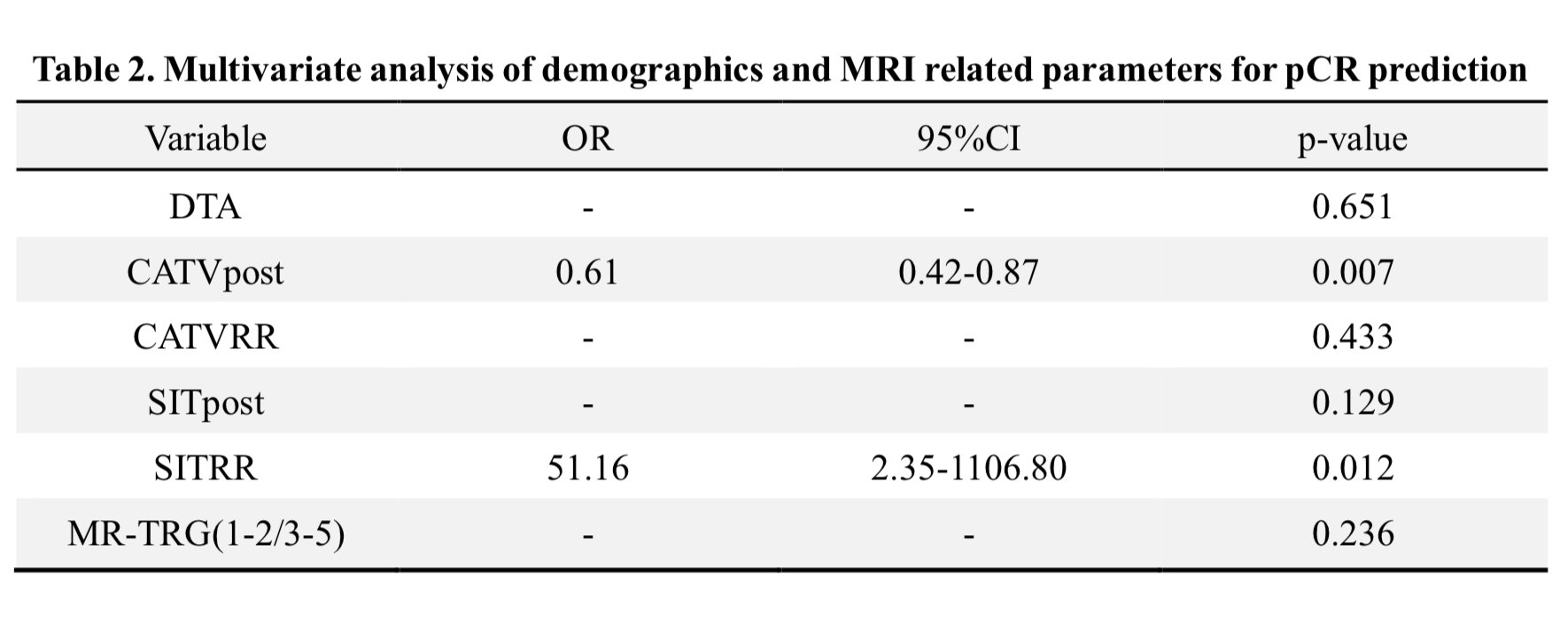
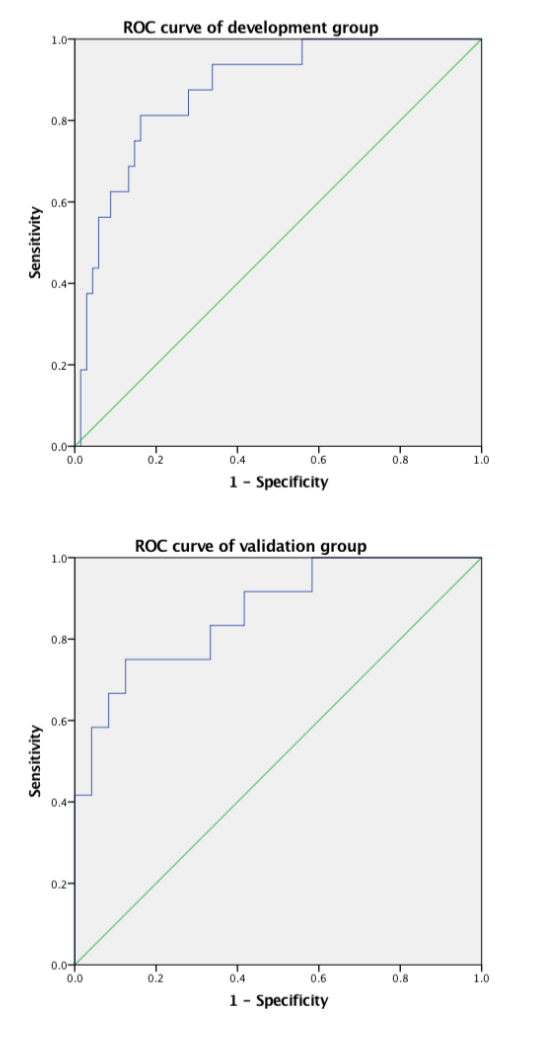
In development and validation group, there were 16 patients (19.0%) and 12 patients (33.3%) achieved pCR respectively. On multivariate analysis, post-nCRT CATV (CATVpost: OR, 0.61; p=0.007) and the reduction rate of SIT (SITRR: OR, 51.16; p=0.012) were independently associated with pCR. The area under the receiver-operating characteristic curve (AUC) for predicting pCR in development group is 0.875(sensitivity 0.813, specificity 0.838) versus in validation group is 0.865(sensitivity0.750, specificity 0.875).
Discussion
Several studies have proven tumor volume measured on T2WI have high diagnostic performance for predicting pCR while another reported tumor signal intensityis good, and one study confirmed that MR-TRG may help. Both of them considered respectively. In our study, all of these parameters were considered comprehensively. Overall, quantitative parameters show more advantages for predicting pCR than qualitative parameters, which may due to poor interreader agreement of qualitative parameters.The AUC of validation group was similar to development group, but lower sensitivity, which may was limited by a small sample size.
Conclusion
This study confirms quantitative parameterssuch as tumor size and signal intensity can help pCR prediction, and CATVpost and SITRRhave better diagnostic efficacy. Further larger studies are required to investigate the clinical applications value of CATVpost and SITRR for “wait-and-see” strategy.Acknowledgements
Fund programs:Special scientific research projects of public health industry(201402019), Beijing science and technology project(Z161100000516101), Beijing hope marathon special fund(LC2016A05)References
1. Van Gijn W, Marijnen CA, Nagtegaal ID, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. The Lancet Oncology2011;12(6):575-82.
2. Kim S, Han K, Seo N, et al. T2-weighted signal intensity-selected volumetry for prediction of pathological complete response after preoperative chemoradiotherapy in locally advanced rectal cancer. European radiology2018.[published online first:2018/06/03]
3. Neri E, Guidi E, Pancrazi F, et al. MRI tumor volume reduction rate vs tumor regression grade in the pre-operative re-staging of locally advanced rectal cancer after chemo-radiotherapy. European journal of radiology2015;84(12):2438-43.
Figures
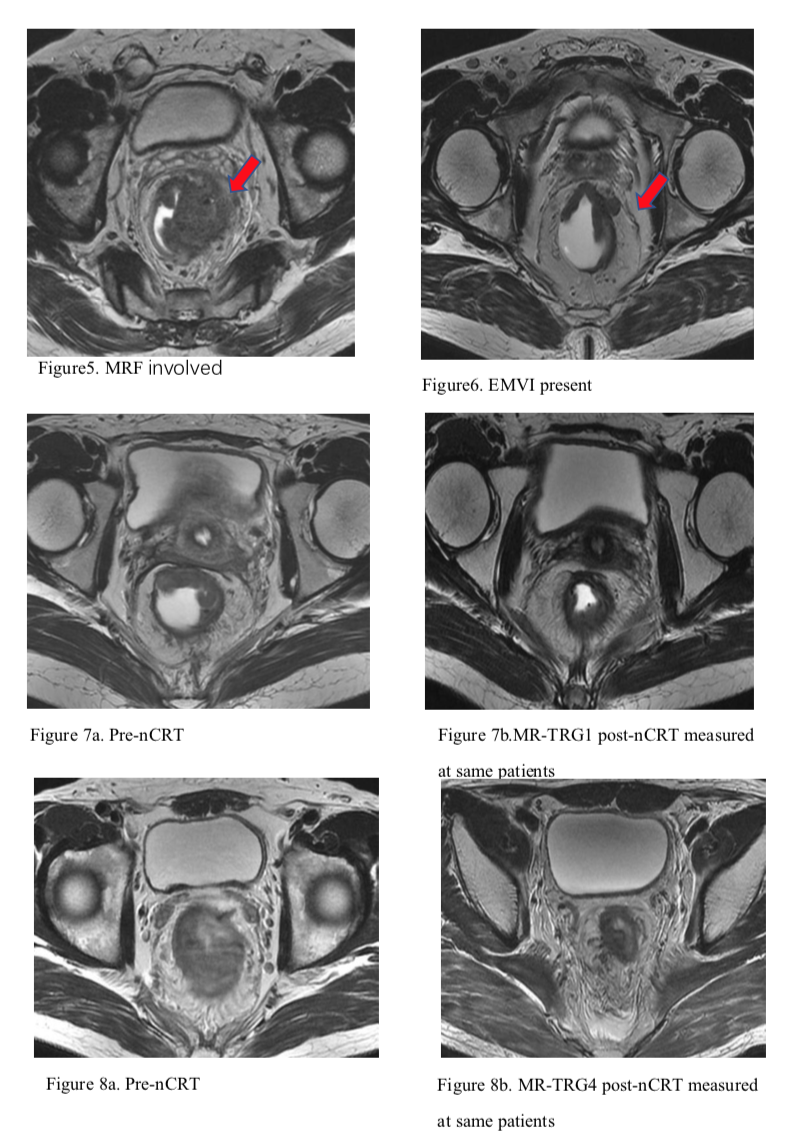
MRF involved: nearest distance between MRF and the tumor≤1mm
EMVI present: EMVI 3-4 score(0-4)
MR-TRG(1)completeregression, theabsence of visible tumorsignal(2)raretumor signal in the context of fibrosis(3)predominantfibrosis but obvious area of tumor signal(4)residualtumor outgrowing fibrosis(5)noregression, theabsence of changes from baseline