2343
Diffusion-weighted MRI for assessing longitudinal effect of radiation (photon beam) versus proton beam therapy on cranial bone marrow in children treated for brain tumors1Cancer Research UK Imaging Centre, The Institute of Cancer Research, Sutton, United Kingdom, 2MRI Unit, The Royal Marsden Hospital NHS Foundation Trust, Sutton, United Kingdom, 3Dept. of Clinical Oncology, The Royal Marsden Hospital NHS Foundation Trust, Sutton, United Kingdom, 4Children's and Young Person's Unit and Haemato-oncology Unit, The Royal Marsden NHS Foundation Trust, Sutton, United Kingdom, 5Department of Neuroradiology, Atkinson Morley Regional Neuroscience Centre, St George's University Hospitals NHS Foundation Trust, London, United Kingdom
Synopsis
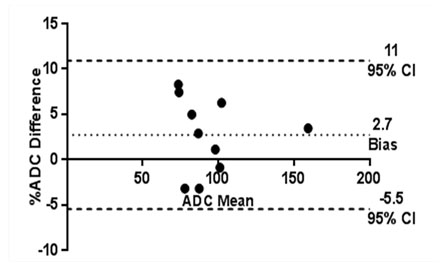
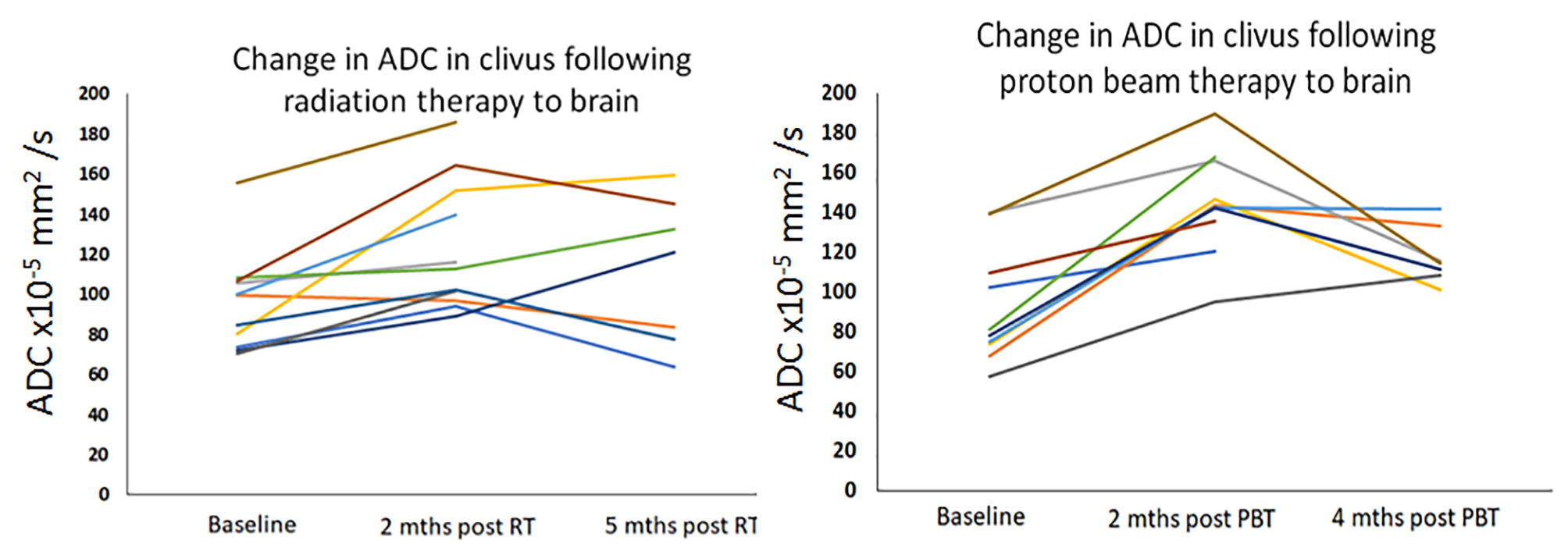
Bone marrow ADC measurements were feasible from the clivus in children. Measurements were reproducible (95% confidence intervals -5.5% to +11%). Following radiation (photon) treatment or proton beam therapy, there was an early rise in ADC at 2 months consistent with bone marrow edema, followed by a fall. The level of early ADC increase (39% for radiation therapy, 42% for proton beam therapy) and pattern of change was similar in both treatment regimens.
Background
Adjuvant Radiotherapy (RT) following surgery is the standard treatment for children with many types of brain tumor. Increasingly, however, proton beam therapy (PBT) is preferred because of its high conformality and potential to reduce late effects1, 2. Effects of RT and PBT on bone marrow are well documented, although hematological toxicity following cranial irradiation is uncommon3 because the amount of bone marrow that is irradiated when treating brain tumors is low. Nevertheless, the skull is a useful region to study the effects of photon and proton beam radiation on pediatric marrow. Diffusion-weighted MRI (DWI) is sensitive to radiation-induced injury to bone-marrow in adults4, but has not been exploited for studying the effects of radiation on the bone marrow in children.Aim
To establish the reproducibility of Apparent Diffusion Coefficient (ADC) measurements derived from paediatric skull bone marrow and compare the effect of conventional (photon) radiotherapy (RT) and proton beam therapy (PBT) on this imaging biomarker in children treated because of a brain tumour.Methods
Reproducibility cohort: 10 patients aged 8-16 years (median 12.9 years) had DWI performed twice to assess reproducibility. Scans were done as part of routine follow-up at least 6 months after RT (6 at the same day visit and 4 after a 1 to 4 month interval)
Treatment effects cohort: Pediatric subjects who had RT at our institution between 2006 and 2017 to treat their central nervous system tumors (or were referred by our institution for PBT) were initially identified. Of 113 children and young adults who had at least two MRI brain scans (one pre- and one post-conventional radiotherapy), 12 were medication free, had not had concomitant chemotherapy, and had DWI scans at all time points that were free from artefact and available for assessment. Of 112 children who had proton therapy, 10 met the same criteria.
Imaging Protocol: T1-W spin-echo axial (slice thickness 5 mm) and coronal (slice thickness 3 mm) pre and post Gadolinium enhancement and sagittal 5mm thick slices post contrast enhancement had been acquired. Additionally, T2-W turbo spin echo, FLAIR and DWI images with b=0 and 1,000 s/mm2 had also been routinely obtained.
ROI delineation: DW images were visually correlated with morphological T2-W images. A circular region of interest of approximately 4-5 mm in diameter was drawn within the clivus (minimum of 20 pixels, range 24 to 129), on two contigugous midline slices of the b=1000 s/mm2 DW images using Adept® software (in-house, The Institute of Cancer Research). ADC was calculated through a monoexponential fit of the data, and ADC maps were created. Descriptive statistics were used to describe the data. Statistical analysis was performed using GraphPad Prism software (version 7.04, GraphPad Incorporated Company, California).
Results
95% confidence intervals of ADC measurements in the reproducibility cohort ranged from -5.5 to +11% (Figure 1). In the treatment effects cohort, 9 out 12 children treated with RT showed an increase in mean ADC values on the first post-treatment scan (mean 60.5 days) of >11% (median 39.2% lower quartile, LQ 23.9%, upper quartile, UQ 54.5%); no decreases below measurement reproducibility were seen. ADC then fell in 5 out 8 patients who had a second follow-up (5 months), but continued to rise in 2, stable in 1 (Figure 2a). In the PBT group, mean ADC increased after treatment above measurement reproducibility in all 10 cases (median 42.4%, LQ 21.1%, UQ 49.2%); at second follow up (4 months), ADC then decreased in 5 of 7 patients scanned, was stable in 1 and rose further in 1 (Figure 2b).Discussion and Conclusions
ADC estimates within the clivus of children are repeatable within a 11% measurement error. Following RT as well as PBT the pattern of ADC change showed an early rise in ADC (at 2 months), followed by a fall in ADC values in the majority of cases. This is in keeping with edema in the bone marrow as a result of acute radiation injury at the early time point. The clivus may be used as a model anatomic area to study the effects of treatment on paediatric bone marrow, as RT and PBT are standard-of-care in children with brain tumors. This pilot data suggests that the pattern and level of change demonstrated was similar with both RT and PBT. The relationship of these changes to radiation dose remains to be established.Acknowledgements
CRUK support to the Cancer Imaging Centre at ICR and RMH in association with MRC and Department of Health C1060/A10334, C1060/A16464 and NHS funding to the NIHR Biomedical Research Centre and the Clinical Research Facility in Imaging.References
1: Munck af Rosenschold P, Engelholm SA, Brodin PN, et al. A Retrospective Evaluation of the Benefit of Referring Pediatric Cancer Patients to an External Proton Therapy Center. Pediatr Blood Cancer. 2016; 63(2):262-9.
2: Stokkevåg CH, Engeseth GM, Ytre-Hauge KS, et al. Estimated risk of radiation-induced cancer following paediatric cranio-spinal irradiation with electron, photon and proton therapy. Acta Oncol. 2014; 53(8):1048-57.
3. Pixberg C, Koch R, Eich HT, et al Acute Toxicity Grade 3 and 4 After Irradiation in Children and Adolescents: Results From the IPPARCA Collaboration. Int J Radiat Oncol Biol Phys. 2016; 94(4):792-9.
4. Lee EYP, Perucho JAU, Vardhanabhuti V, et al. Intravoxel incoherent motion MRI assessment of chemoradiation-induced pelvic bone marrow changes in cervical cancer and correlation with hematological toxicity. J Magn Reson Imaging. 2017; 46(5): 1491-1498.
Figures