2338
Change of Radiotherapy Planning Target Volume Delineated on Pre-Treatment and mid-RT Follow-up MRI After 3-4 Weeks of TreatmentYang Zhang1, Liming Shi2, Xiaonan Sun2, Tianye Niu2, Ning Yue3, Jeon-Hor Chen1,4, Tiffany Kwong1,3, Min-Ying Lydia Su1, and Ke Nie3
1Department of Radiological Sciences, University of California, Irvine, CA, United States, 2Department of Radiation Oncology, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, China, 3Department of Radiation Oncology, Rutgers-The State University of New Jersey, New Brunswick, NJ, United States, 4Department of Radiology, E-Da Hospital and I-Shou University, Kaohsiung, Taiwan
Synopsis
As tumor shows substantial shrinkage over the course of treatment, should radiation treatment volume be adjusted? A quantitative method using “radial distance”- the distance from the outer boundary of the tumor to the center of the rectum, was developed to evaluate the gross tumor volume (GTV) delineated on MRI acquired before treatment and after 3-4 weeks of radiation. In 35 patients, the mean tumor volume decreased from 19.1 to 10.5 cm3 but the mean radial distance only decreased slightly from 16.3 to 15.6 mm. When the remaining tumor was close to the rectal wall, the PTV should not be adjusted.
Introduction
The development of conformal radiation techniques such as intensity modulated radiotherapy (IMRT) or volumetric modulated arc therapy (VMAT) opens up opportunities for delivering higher dose boosts, which have been shown to improve treatment efficacy and achieve better pathological response [1-4]. This challenging technique requires sophisticated planning and precise estimation of the tumor boundary and treatment field to achieve a satisfactory treatment efficacy and minimize side effects. With the advancement of fast acquisition of MRI scans and the possibility to obtain reliable electron density, MRI-guided treatment planning and MRI-linear accelerator (LINAC) treatment systems are gradually gaining popularity in radiotherapy. MRI shows much better soft tissue contrast than CT, which can lead to better lesion delineation. The current standard-of-care treatment for patients with locally advanced rectal cancer is neoadjuvant chemoradiation therapy (CRT) followed by surgery. It is known that most patients would respond to CRT and show substantial tumor shrinkage. Conventionally, the planning target volume (PTV) is determined before the start of CRT and the same PTV is used over the entire course and do not account for changes in the tumor volume. Whether the planning field needs to be changed, or how much adjustment needs to be made, has never been studied before, which can be investigated using the tumor delineated on pre-treatment MRI and follow-up MRI after 3-4 weeks of radiation treatment. In order to evaluate the changes, a quantitative method using “radial distance” was developed to evaluate the change of treatment field with tumor shrinkage after the start of CRT.Methods
A total of 35 patients (mean age 59) with locally advanced rectal cancer receiving CRT were included in this study. The preoperative CRT included 50 Gy delivered for 25 fractions in 5 weeks using the IMRT technique with concomitant chemotherapy. Each patient had two MRI, one at 1-2 weeks before treatment, and another at 3-4 weeks after the start of radiation treatment. MRI was performed on 3T, using a multi-parametric protocol including T1, T2, DWI, and DCE using the LAVA sequence with 4 frames, L1 before contrast injection, and L2, L3, L4 at 15s, 60s, and 120s after injection. The tumor was manually outlined on post-contrast images L2 or L3 by an experienced radiologist. The total tumor volume was calculated. A radial distance method was developed to quantitatively measure the distance from the outer boundary of the tumor to the center of the rectum to evaluate the radiation treatment zone. A body radiologist chose one middle slice and manually traced the rectum contour, then it was used as reference for Demon algorithm to segment the rectum on adjacent slices. The segmentation of rectum and tumor is illustrated in two cases shown in Figure 1. The measurement of radial distance is shown in Figure 2, defined as the distance from the centroid of the segmented rectum on each slice to the last intersecting point on the tumor ROI boundary in the radial direction. A total of 180 radial lines at 2° interval were used, and only the lines intersecting with the outer tumor boundary were included in the analysis (noted as tumor boundary pixel). The mean radial distance was calculated by averaging the RD over all tumor boundary pixels. For each patient, the change in the tumor volume and mean RD between the pre-treatment and mid-RT follow-up MRI was calculated.Results
Of all 35 patients, the mean tumor volume showed a large decrease, from 19.1 ± 14.5 cm3 to 10.5 ± 11.1 cm3. The mean of the total number of tumor boundary pixels from 35 patients was 1,475 in pre-treatment MRI, and decreased to 886 in the mid-RT follow-up MRI. Despite the obvious tumor volume shrinkage and the decreased number of tumor boundary pixels, the difference in the mean RD was very small, only decreasing from 16.3 ± 2.8 mm to 15.6 ± 3.6 mm. Figure 3 shows the waterfall plot of the percentage change in tumor volume of 35 patients, i.e. by sorting the changes from the smallest to the greatest and plotting them in a sequential order (Figure 3A), as well as the percentage change in the mean RD for each corresponding patient (Figure 3B). It is clearly seen that although the tumor shrinks substantially, the mean RD does not decrease proportionally. Figure 4 shows one patient with decreased tumor volume and decreased tumor RD. Figure 5 shows another patient with decreased tumor volume but, in contrast, increased tumor RD, because the residual tumor was at the outer boundary of the tumor close to the rectum.Discussion
Over the course of CRT, tumor shrinkage is expected; nonetheless, the same radiation planning target volume delineated based on the original tumor bed before radiation is used throughout the treatment course. In this study, MR imaging was performed before CRT and 3-4 weeks after starting treatment, which allowed us to evaluate the change of radiation treatment planning zone. Our results show that the overall tumor volume was decreased by 45%, consistent with findings by Van den Begin et al. [5], but the mean radial distance of the tumor was similar between pre-treatment and mid-RT follow-up MRI. The results show that the shrinkage of rectal cancer does not follow a specific pattern, and that the decrease in tumor volume is not corresponding to the change in the radial distance, which is a much more relevant parameter for RT treatment. Therefore, although the overall tumor volume is decreased, the small decrease in the mean radial tumor distance suggests that the same PTV should be used for the entire course of radiation therapy despite substantial tumor shrinkage over time.Acknowledgements
This study was supported in part by NIH R01 CA127927, the Rutgers Cancer Institute of New Jersey (No. P30 CA072720), Chinese National Natural Science Foundation (No. 81441086, 81672976), Natural Science Foundation of Zhejiang Province (No. LY14H160016), Major Science and Technology Program of Zhejiang Province (No. 2013C03044-6).References
[1] Kye et al. Overview of radiation therapy for treating rectal cancer. Annals of coloproctology 30(4), 165-174 (2014). [2] Smith et al. Advances and challenges in treatment of locally advanced rectal cancer. Journal of clinical oncology 33(16), 1797-1808 (2015). [3] Burbach et al. Impact of radiotherapy boost on pathological complete response in patients with locally advanced rectal cancer: a systematic review and meta-analysis. Radiotherapy and Oncology 113(1), 1-9 (2014). [4] Burbach et al. RandomizEd controlled trial for pre-operAtive dose-escaLation BOOST in locally advanced rectal cancer (RECTAL BOOST study): study protocol for a randomized controlled trial. Trials 16(1), 58 (2015). [5] Van den Begin et al. Tumor volume regression during preoperative chemoradiotherapy for rectal cancer: a prospective observational study with weekly MRI. Acta Oncologica 57(6), 723-727 (2018).Figures

Figure 1.
Top Panel: An 80-year-old male patient with low-rectum cancer at stage of
cT3N2M0. Images from 6 tumor-containing slices, with segmented rectum (in
green) and manually drawn tumor ROI (in red), are shown. Bottom Panel: A
73-year-old female patient with mid-rectum cancer at stage of cT3N0M1, showing different
shape of rectum and smaller tumor.

Figure
2. (A,D) Pre-contrast Images; (B,E) L2
Post-contrast images; (C,F) Rectum contour (green) with tumor (red) to
illustrate the radial distance (orange) for two case examples. The distance
from the centroid of the rectum to the farthest pixel on the tumor ROI boundary
in the radial direction is defined as the radial distance, marked in the
figure.

Figure
3. (A) The waterfall plot of percent change in
tumor volume of 35 patients between the pre-treatment and mid-RT follow-up MRI
studies. (B) The corresponding percentage change in the mean radial distance.
The images of patient #13 is shown in Figure
4, denoted by (*) symbol, who shows -36% tumor volumetric reduction and
decreased RD from 12.4 mm in pre-treatment to 7.7 mm in mid-RT MRI, -38%. The
images of patient #26 is shown in Figure
5, denoted by (†) symbol, who has -73 % tumor volumetric
reduction, but increased mean RD from 3.9 to 5.2 cm, +33%.

Figure 4. Example of rectum and tumor segmentation on L2 post-contrast images of a 56-year-old male patient with low-rectum cancer at stage of cT2N2M0 (Patient #13). Top row shows segmented rectum (green) and the manually drawn tumor ROI (red) before starting treatment on 4 imaging slices. The bottom row shows the corresponding tumor on 4 slices after 3 weeks of CRT, clearly showing tumor shrinkage. The tumor volume is 33.9 cm3 in pre-treatment MRI, 21.6 cm3 in mid-RT MRI, showing -36% reduction. The total number of tumor boundary pixels is 2,513 in pre-treatment, and 2,106 in mid-RT MRI. The mean RD is 12.4 mm in pre-treatment, 7.7 mm in mid-RT MRI, showing -38% reduction.
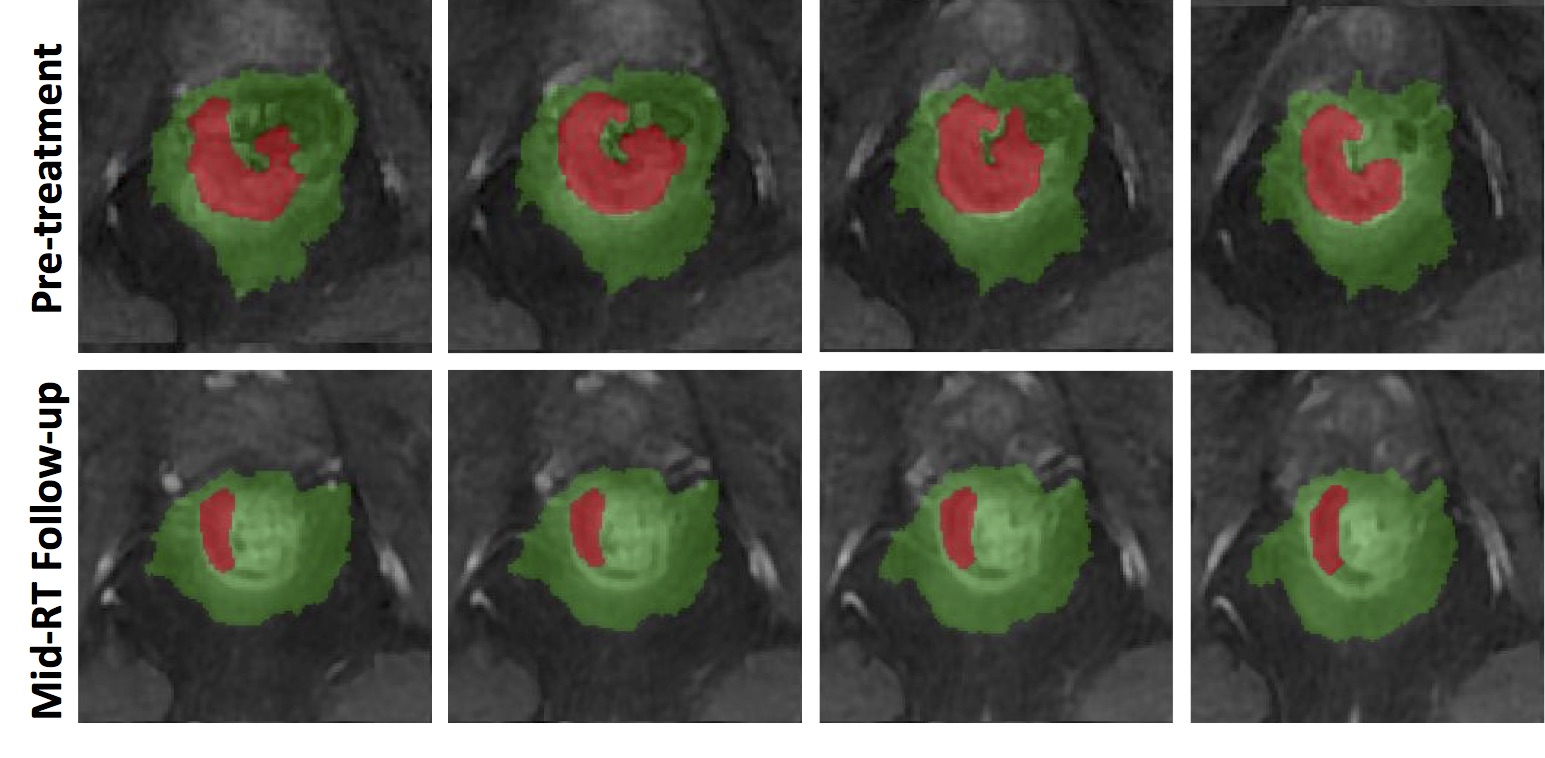
Figure
5. The pre-treatment and mid-RT follow-up MRI of
patient #26, showing substantial volumetric shrinkage but increased mean RD.
For this patient, the tumor volume is 9.2 cm3 in pre-treatment MRI, and
decreases to 2.5 cm3 in mid-RT, showing -73% reduction. The total
number of tumor boundary pixels is 966 in pre-treatment, and 455 in mid-RT MRI. However, the mean RD in pre-treatment
MRI is 3.9 cm and that increases to 5.2 cm in mid-RT MRI, +33%. As seen in the
figure, the remaining tumor after 3-4 weeks of RT is in the outer region of the
original tumor bed close to the rectal wall. Therefore, although the tumor
shows substantial shrinkage, the mean RD does not decrease, and the radiation
treatment zone should not change.