2328
Respiratory motion characterization and motion uncertainty estimation using a fast 3D+t MRI and bootstrapping for abdominal radiotherapy1Medical Physics and Research Department, Hong Kong Sanatorium & Hospital, Hong Kong, Hong Kong
Synopsis
Respiratory motion characterization and uncertainty estimation is important in radiotherapy treatment
Introduction
Radiotherapy (RT) treatment planning of the abdomen is often challenged by the pronounced respiratory motion. Probabilistic treatment planning provides a patient-specific motion management solution by including the respiratory-induced tumor motion in the treatment planning optimization processing [1]. Although a few preliminary studies showed limited dosimetric benefit by using probabilistic treatment planning [1], it was partially attributed to the limitations in respiratory motion characterization and its uncertainty estimation, restricted by the imaging capability of 4DCT or time-resolved single/multi-slice MRI (2D+t). Time-resolved volumetric MRI (3D+t MRI) has recently been proposed to overcome the limitations of 4DCT or 2D+t MRI by (1) its superior soft-tissue contrast [2,3], and (2) its prospective and simultaneous 3D motion capturing with sufficiently high temporal resolution. Moreover, respiratory motion uncertainty is postulated to be better estimated by motion tensor analysis and bootstrapping technique. We, thus, proposed to better characterize the positional and orientation uncertainty of abdominal organ motion during free-breathing using 3D+t MRI, bootstrapping and tensor analysis.Methods
Free-breathing upper abdominal 3D+t MR images were obtained on 9 healthy volunteers (age: 36±6) using a 3D-spoiled gradient-echo sequence (transversal, FOV=350(FE)x262.5(PE)mm, matrix size=128x128x56, thickness=4mm, TE/TR=0.53/1.57ms, flip-angle=5o , RBW=1400Hz/voxel, CAIPIRINHA factor=4, partial Fourier factor=6/8, 144 timeframes) at 1.63 frame-per-sec (fps) on a 1.5T MR-simulator with a 18-channel body matrix coil and spine coil. Liver, left kidney, right kidney and spleen were segmented on the first timeframe, and their motions were estimated by rigidly registering the image volumes to the chronologically first timeframe. For each image set, the estimated positional shift was subtracted by the mean positional shift prior to the generation of 1000 bootstrap samples through bootstrapping. For each bootstrap sample, the covariance matrix was calculated for the generation of the corresponding eigenvalues (λ1, λ2, λ3) and eigenvectors (v1, v2, v3) using single value decomposition (i.e. 1000 sets of eigenvalues and eigenvectors in total). The mean principle eigenvector was subsequently estimated using the mean dyadic tensor (i.e.$$$\frac{1}{1000} \sum_{i=1}^{1000} v_{1} v^{T}$$$ ). The uncertainty of the principle eigenvector orientation was evaluated using the apex angle of the cone of uncertainty (aCU, the angle between the mean principle eigenvector and each bootstrap estimate of principle eigenvector).Results
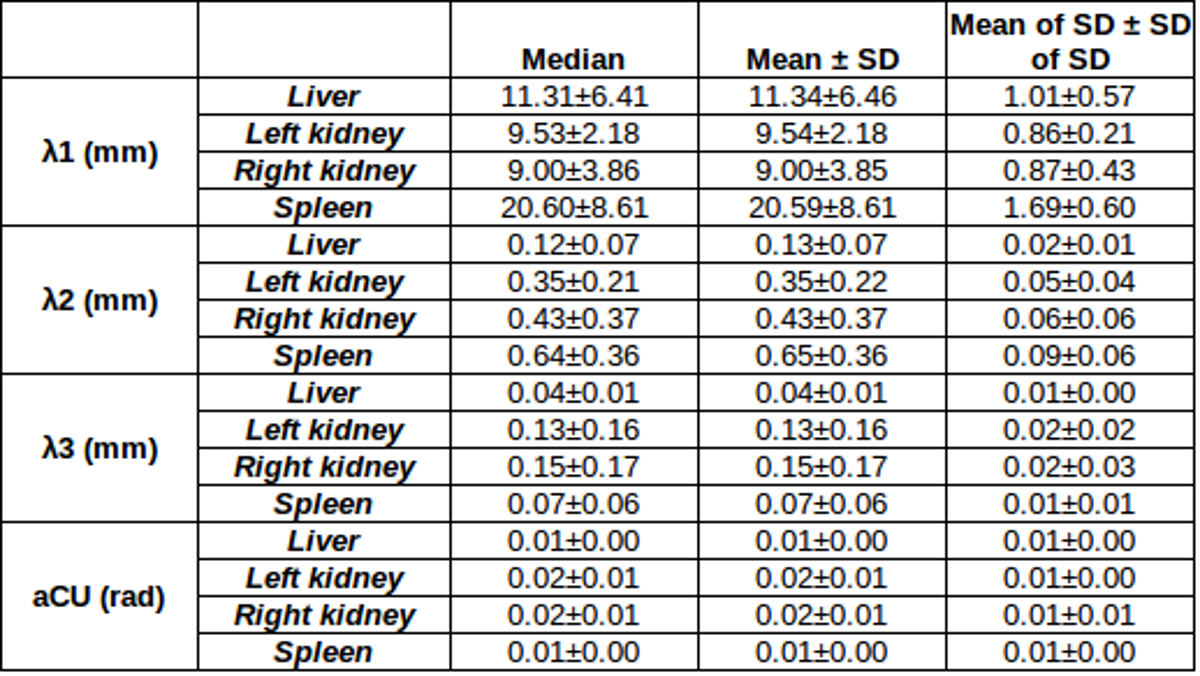
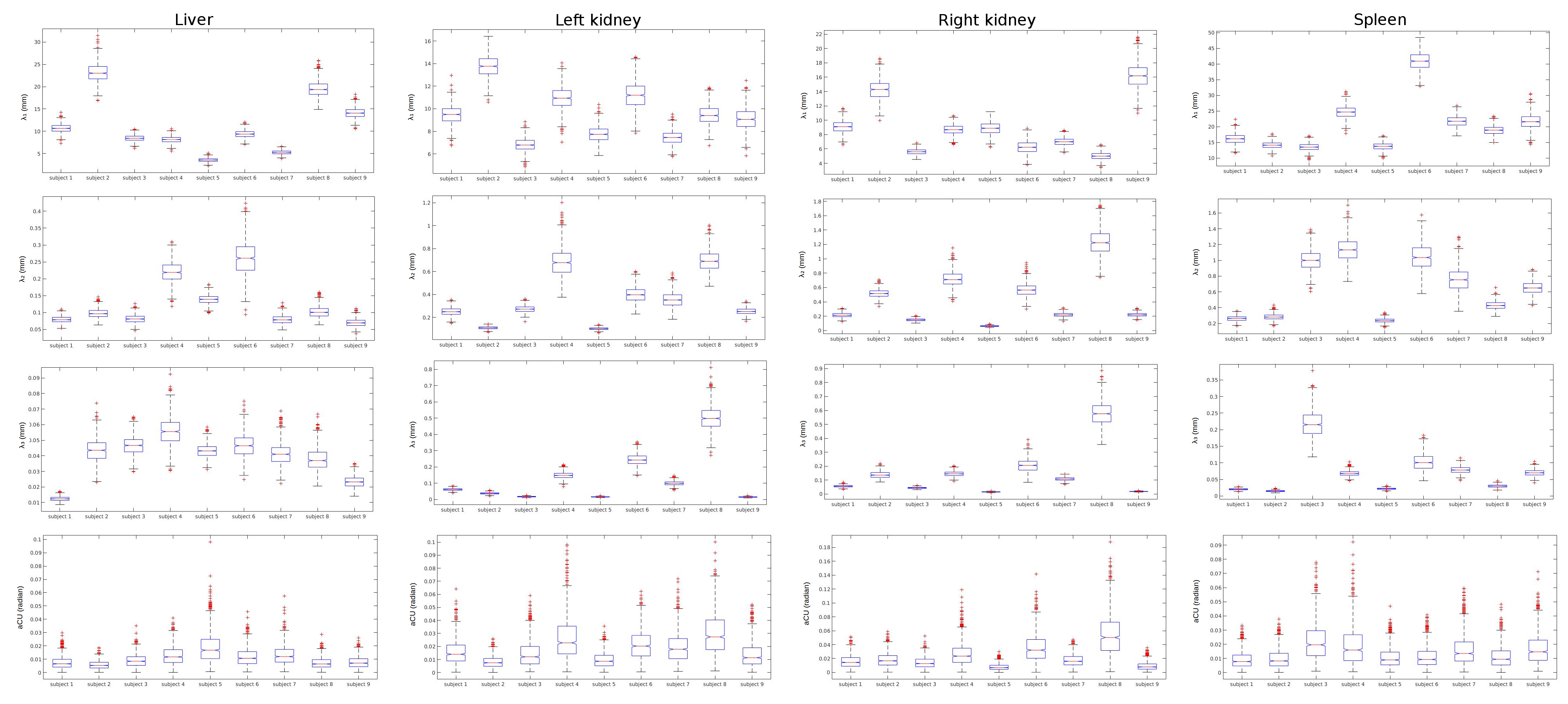
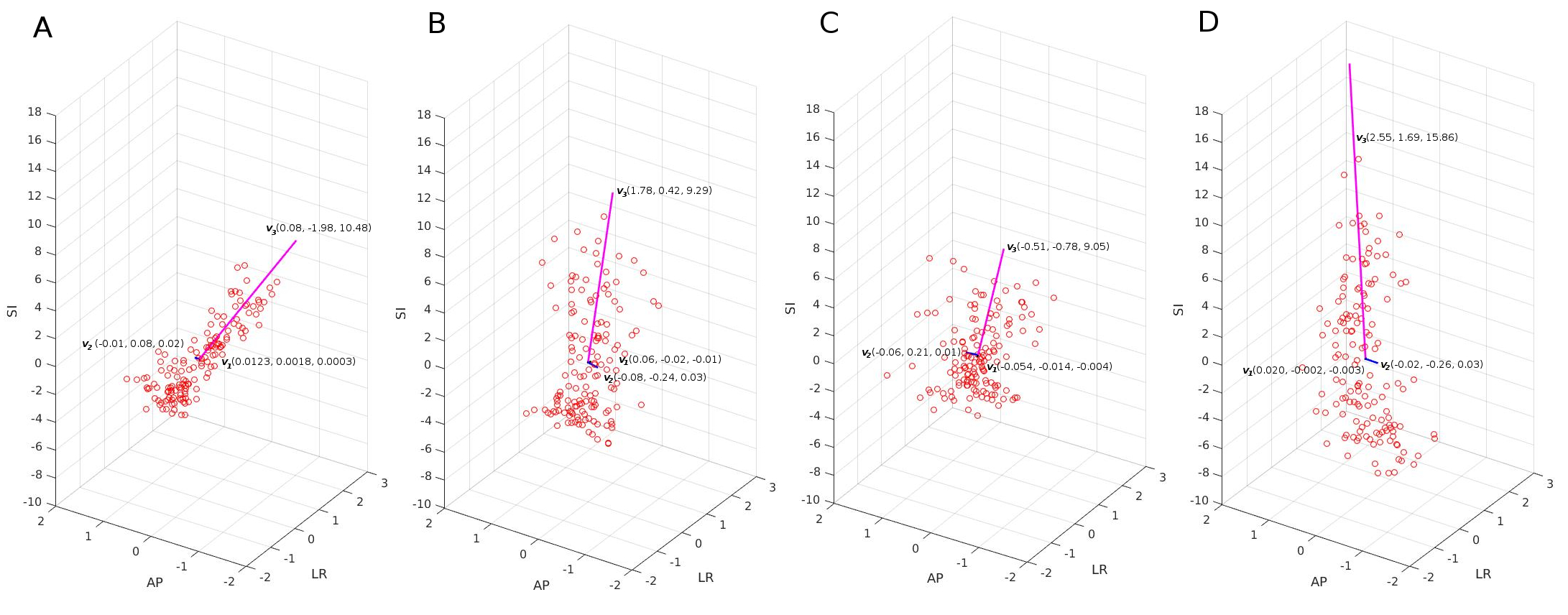
The mean eigenvectors(v1, v2, v3) with the length of the corresponding mean eigenvalues (λ1, λ2, λ3) of the respiratory organ position in a subject were illustrated in Figure 2. The mean and median of λ1, λ2, λ3 and aCU were shown in Table 1. For all organs, the mean aCU was small (< 0.01 radian (0.57o)). The largest mean λ1 and λ2 were obtained in the spleen (λ1 = 20.59±8.61mm, λ2 = 0.65±0.36mm) when compared with other organs (λ1 = 11.34±6.46mm (liver), 9.54±2.18mm (left kidney), 9.00±3.85mm (right kidney) , λ2 = 0.13±0.07mm (liver), 0.35±0.22mm (left kidney), 0.43±0.37mm (right kidney)).Discussion
The stability of the probabilistic organ position distribution in the respiratory motion is mainly affected by the breathing irregularity, while could still subject to the imaging limitations in spatial and temporal resolution as well as registration error. The small aCU (<0.01 radian (0.57o)) obtained in this study suggests that the current 3D+t MRI protocol was fast enough for respiratory motion sampling, thus allowed a reliable estimation of the respiratory-induced organ motion. We believed that our estimation might better represent respiratory motion than the traditional methods by taking the advantage of the high temporal resolution of 3D+t MRI in that (1) our tensor-based estimation was rotationally invariant so, theoretically, independent of patient positioning and more reliable; (2) orientation uncertainty estimation, which was rarely investigated, might provide additional information on the respiratory motion for probabilistic treatment planning. For all organs, our estimated λ1 was much larger than λ2 and λ3, which mainly reflected the expected largest positional shift along SI (Figure 2). The λ1 of the left (9.54±2.18mm) and right kidneys (9.00±3.85mm) were similar to the reported SI displacement (left kidney: 8.48±3.04mm; right kidney: 8.9±3.7mm) [4]. It was worth noting that a larger λ1 in liver than in spleen were observed, probably due to the large deformability of liver during respiration. As such, further study using non-linear registration is warrant. Other limitation of this study includes a small sample size and short scan time (relative to the typical radiotherapy treatment).Acknowledgements
No acknowledgement found.References
[1] Lens E, Kotte AN, Patel A et al. Probabilistic treatment planning for pancreatic cancer treatment: prospective incorporation of respiratory motion shows only limited dosimetric benefit. Acta. Oncol. 2017; 56(3): 398-404
[2] Schmidt MA, Payne GS. Radiotherapy planning using MRI. Phys Med Biol 2015; 60(22): R323-361
[3] Biederer J, Hintze G, Fabel M et al. Magnetic resonance imaging and computed tomography of respiratory mechanics. J Magn Reson Imaging 2010; 32(6): 1388-1397
[4] Song R, Tipirneni A, Johnson P et al. Evaluation of respiratory liver and kidney movements for MRI navigator gating. J Magn Reson Imaging 2011; 33(1): 143-148
Figures