2323
PET/MRI versus PET/CT in Oncology: A Prospective Single-center Study Focusing on Implications for Patient Management and Cost ConsiderationsMarius Erik Mayerhoefer1,2, Helmut Prosch3, Lucian Beer3, Dietmar Tamandl3, Thomas Beyer3, Ivo Rausch3, Dominik Berzaczy3, Markus Raderer3, Christoph Hoeller3, Matthias Preusser3, Ahmed Ba-Ssalamah3, Georgios Karanikas3, Julia Kesselbacher3, Gerald Prager3, Michael Weber3, Bernhard Brauner4, Markus Mitterhauser3, Harald Eidherr3, and Alexander Haug3
1Medical University of Vienna, Wien, Austria, 2Memorial Sloan Kettering Cancer Center, New York, NY, United States, 3Medical University of Vienna, Vienna, Austria, 4Siemens Healthineers, Vienna, Austria
Synopsis
To prospectively investigate the clinical impact of PET/MRI, compared to PET/CT, in a mixed population of cancer patients, and to perform an economic evaluation of PET/MRI. 263 patients (330 same-day PET/CT and PET/MRI examinations) were analyzed. PET/MRI was accurate in 319/330 examinations, and PET/CT in 277/330 examinations; respective accuracies (97.3% vs. 83.9%) differed significantly (P<0.001). Additional findings on PET/MRI had implications for clinical management in 21/263 patients (8.0%). Incremental cost-effectiveness ratios for PET/MRI were 22.47 EUR (~26.28 USD) per percent of diagnostic accuracy, and 37.64 EUR (~44.06 USD) per percent of correctly managed patients.
INTRODUCTION:
PET/MRI (positron emission tomography / magnetic resonance imaging) is a relatively novel hybrid imaging technique that is potentially superior to PET/CT, the standard hybrid imaging test for cancer patients, while offering reduced radiation exposure. Therefore, it was our aim to prospectively investigate the clinical impact of PET/MRI (positron emission tomography / magnetic resonance imaging), compared to PET/CT (computed tomography), in a mixed population of cancer patients, and to perform an economic evaluation of any perceived clinical benefit of PET/MRI.METHODS:
Patients with histologically-proven cancers that were referred for routine staging or follow-up by PET/CT, were eligible for inclusion in this IRB-approved prospective study. Patients underwent PET/CT (with contrast-enhanced CT), and immediately after it, PET/MRI, using [18F]FDG, [68Ga]DOTANOC, or [18F]DOPA, depending on histology. PET/MRI included an axial, two-point 3D VIBE Dixon, a coronal T2 HASTE, an axial free-breathing SPAIR DWI (b50, b800), and a gadolinium-enhanced T1 VIBE fat sat sequence. PET/MRI and PET/CT were rated separately, and lesions were assessed per anatomic region; based on regions, per examination and per patient analyses were performed. A simulated, multi-disciplinary tumor board (MTB) decided whether differences between PET/CT and PET/MRI would affect management. Subsequently, and with access to all clinical, histological and imaging data (including follow-up CT, MRI, PET/CT, or PET/MRI), the MTB also served as reference standard. McNemar tests were used to compare examination-based accuracies, and incremental cost-effectiveness ratios (ICER) for PET/MRI, based on examination-based accuracies and changes in management, were calculated.RESULTS:
A total of 263 patients were analyzed: same-day PET/CT and PET/MRI after a single radiotracer injection was performed once in 221 patients; twice in 27 patients; at three time points in 10 patients; at four time points in five patients; and at five time points in one patient. Thus, a total of 330 same-day PET/CT and PET/MRI examinations (staging; 169; restaging, 161) were available for further analysis. The largest cancer groups were lymphoma (52 patients); non-small cell lung cancer (NSCLC; 46 patients); well-differentiated neuroendocrine tumors (35 patients); melanoma (26 patients); pancreatic adenocarcinoma (16 patients); and cancer of unknown primary (13 examinations). PET/MRI was accurate in 319/330 examinations, and PET/CT in 277/330 examinations; the respective accuracies of 97.3% and 83.9% differed significantly (P<0.001). The additional findings on PET/MRI (most of them liver and brain metastases in patients with NSCLC, melanoma, and neuroendocrine tumors; see Fig. 1) had implications for clinical management in 23/330 examinations (7.0%), and 21/263 patients (8.0%). On the other hand, none of the additional findings that were observed on nine PET/CT examinations, but not on PET/MRI – all of which were lung metastases – had implications for clinical management or therapy. The total cost of ownership for 10 years was calculated as 12.3 million EUR (~14.4 million USD) for PET/MRI, and 10.2 million EUR (~11.9 million USD) for PET/CT. The number of examinations within these 10 years was calculated as 20,000 (10 * 250 workdays/year * 8 examinations/day) for PET/MRI, and 32,500 (10 * 250 workdays/year * 13 examinations/day) for PET/CT. Based on these numbers, the average unit cost per examination was calculated as 615 EUR (~719 USD) for PET/MRI and 313.85 EUR (~367 USD) for PET/CT. Consequently, ICERs for PET/MRI were 22.47 EUR (~26.28 USD) per percent of diagnostic accuracy, and 37.64 EUR (~44.06 USD) per percent of correctly managed patients.DISCUSSION:
The results of our prospective study suggest that PET/MRI provides additional clinical value in terms of changes to more appropriate management in 8% of cancer patients that undergo PET/CT in routine clinical practice. Notably, this percentage is lower than in the largest study so far: with regard to implications for clinical management, Catalano et al reported an overall superiority of PET/MRI over PET/CT for 16% of cancer patients in their retrospective analysis [1]. This discrepancy can possibly be explained by the differences in relative frequencies of cancer histologies between our study and the Catalano study (e.g., NSCLC, 17% vs. 7%; melanoma, 10% vs. 3%; breast cancer, 2% vs. 26%; or colorectal cancer, 3% vs. 11%; of the entire respective cohorts). While our results clearly do not justify a general replacement of PET/CT with PET/MRI, they, however, do suggest that certain subgroups – such as advanced-stage NSCLC and melanoma – could benefit from undergoing PET/MRI instead of PET/CT.CONCLUSION:
The choice of PET/MRI over PET/CT enables more appropriate management in a non-negligible percentage of patients. Since PET/MRI is almost twice as cost-intensive as PET/CT, a histology-based triage of patients to either PET/MRI or PET/CT may be meaningful.Acknowledgements
No acknowledgement found.References
1. Catalano OA, Rosen BR, Sahani DV, Hahn PF, Guimaraes AR, Vangel MG, Nicolai E, Soricelli A, Salvatore M. Clinical impact of PET/MR imaging in patients with cancer undergoing same-day PET/CT: initial experience in 134 patients—a hypothesis-generating exploratory study. Radiology. 2013 Dec;269(3):857-69.Figures
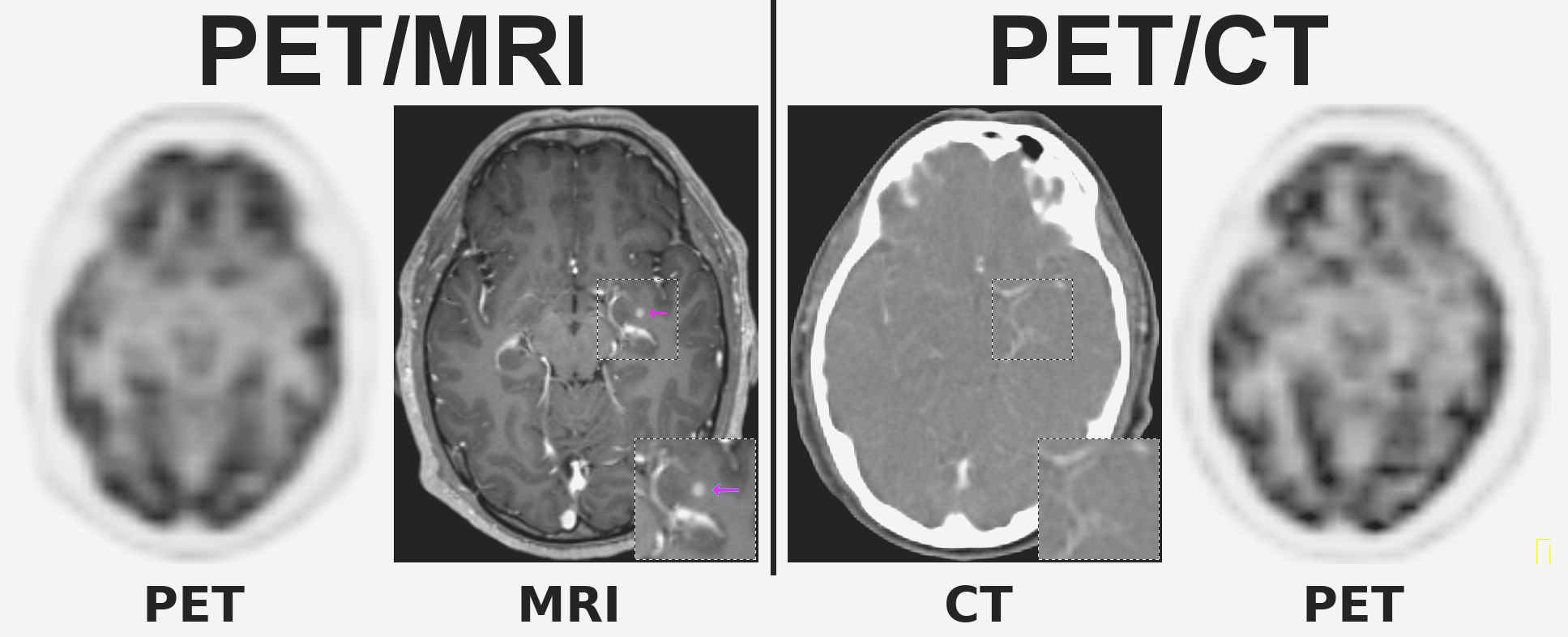
Figure 1: A 61-year-old patients with melanoma stage IV,
referred for staging before nivolumab treatment. While [18F]FDG-PET is
unremarkable for both PET/MRI and PET/CT, the contrast-enhanced MRI
component of PET/MRI depicts a small brain metastases in the left
hippocampus (pink arrow) that is not visualized on the contrast-enhanced
CT component of PET/CT (see also 1.5x magnifications of the region in
the right lower corners), and for which radiation therapy is indicated.