2322
PET/MRI as a sensitive diagnostic tool for peritoneal carcinomatosis: early results from a single center prospective study1Translational and Molecular Imaging Institute, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 2Department of Radiology, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 3Radiology, Lausanne University Hospital, Lausanne, Switzerland, 4Department of Surgery, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 5Department of Nuclear Medicine, Icahn School of Medicine at Mount Sinai, New York, NY, United States
Synopsis
The goal of our study was to assess the diagnostic value of PET/MRI for diagnosis and spatial localization of peritoneal carcinomatosis (PC) in patients prior to potential cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC). We found that PET/MRI is sensitive and accurate at predicting PC at the patient level as compared to surgery, the reference standard. However, PET/MRI was not to as accurate in localizing PC in the abdominopelvic cavity. Findings need to be validated in a larger study.
Purpose
PC is an advanced malignant disease with a poor prognosis for which CRS and HIPEC can be used as treatment.1 PC is evaluated surgically using Sugarbaker’s peritoneal cancer index (PCI).2 Current imaging methods show that radiological PCI correlates well with surgical PCI3 with good sensitivity and specificity.4 PET/MRI is a relatively new modality that is not widely used to estimate PCI. The goal of our study was to assess the diagnostic value of PET/MRI for diagnosis and spatial localization of PC.Methods
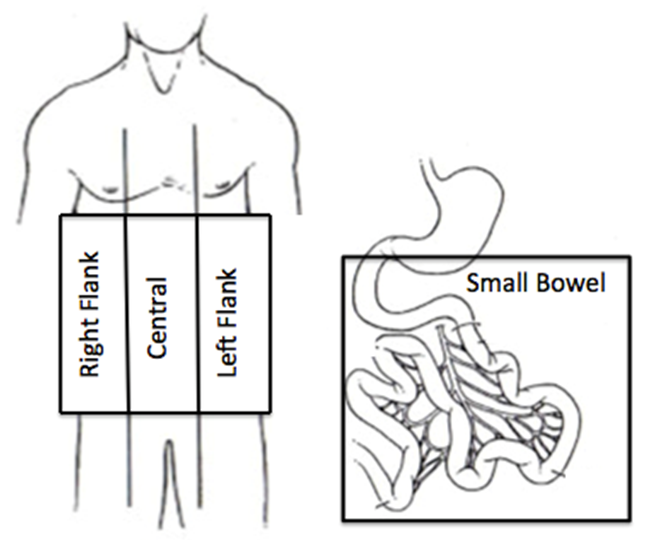
This IRB approved prospective single center study included 12 patients with suspected PC (M/F 3/9, mean age 57y, primary cancer: colon=6, appendiceal=3, ovarian=1, mesothelioma=1, gallbladder=1) who had FDG-PET/MRI prior to surgery. The study was performed on a 3T PET/MRI system (Biograph mMR, Siemens). The MRI protocol included axial and coronal HASTE, axial T1 in-and-out of phase, axial DWI, axial and coronal VIBE pre- and post-contrast. Simultaneous PET acquisition was done. Two blinded observers (one nuclear medicine physician and one Body MRI radiologist) evaluated PET, DWI, and contrast enhanced (CE) T1W images. The abdominopelvic cavity was divided into 4 regions: right flank, central, left flank, and small bowel, modified from Sugarbaker’s PCI scheme of 13 sections (Figure 1).2 Using Sugarbaker’s lesion size (LS) score criteria, each region was assigned a score from 0-3 based on the size of the largest peritoneal implant found: LS 0 (no tumor seen), LS 1 (tumor up to 0.5 cm), LS 2 (tumor up to 5.0 cm), and LS 3 (tumor greater than 5.0 cm or confluence). Combining the study data created PET/MRI region scores and PCI. Surgical PCI was documented intraoperatively and was also modified into 4 abdominopelvic regions, with assigned LS score of each region ranging from 0-3.
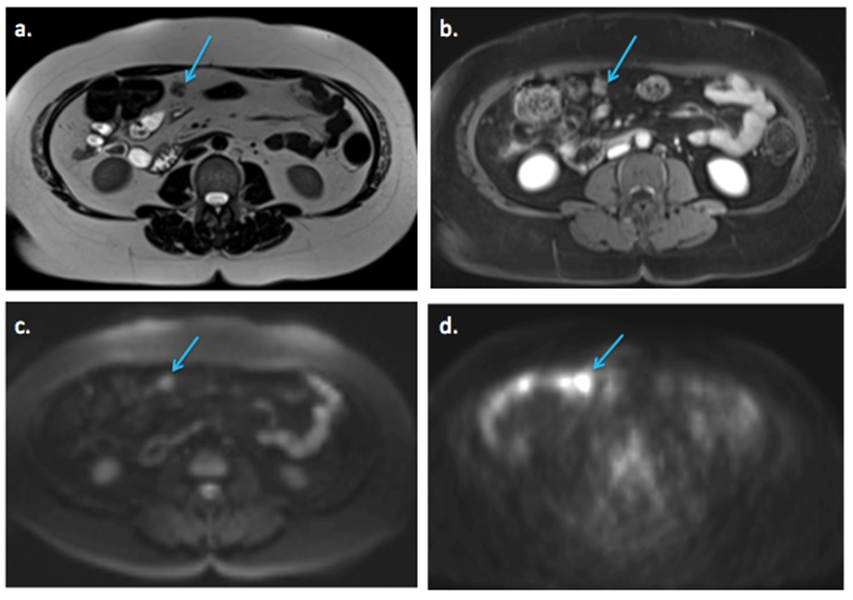
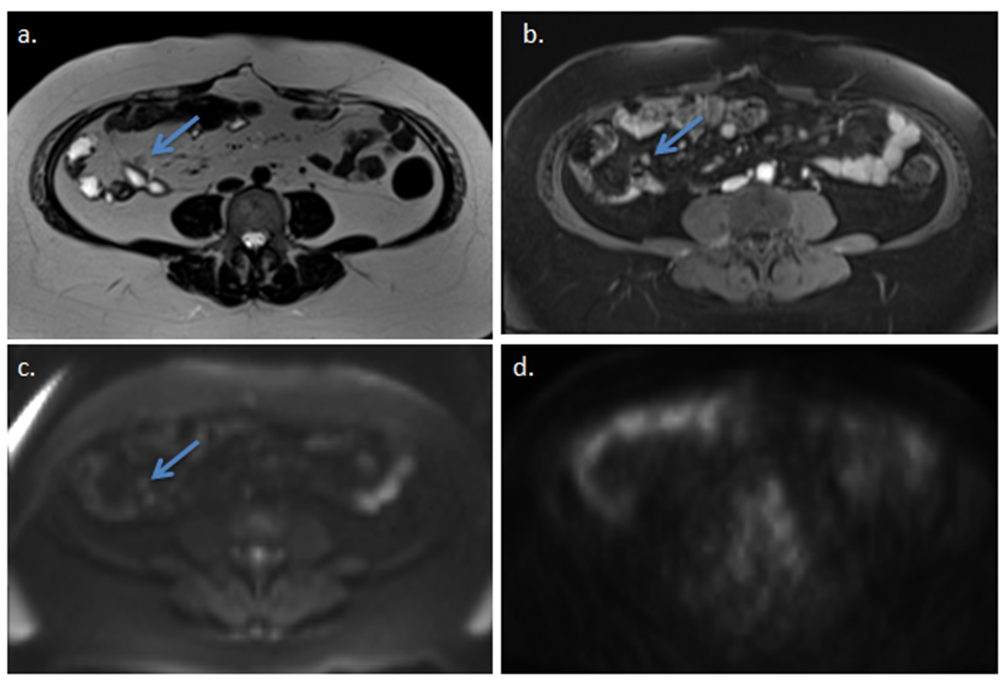
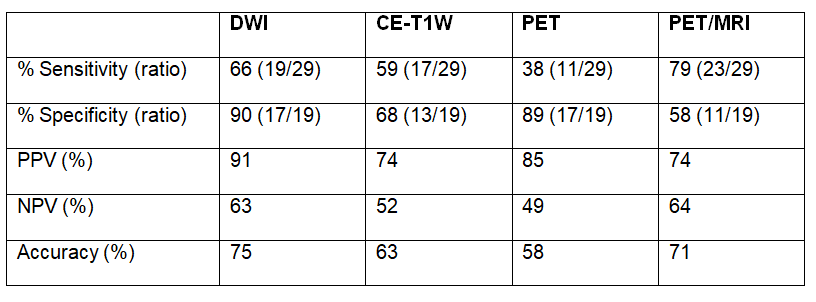
Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated at patient and region levels. A true positive per region was defined as presence of any peritoneal disease (score 1-3) on both the imaging modality and at surgery (Figures 2,3). True negative per region was defined as no detectable disease on both imaging and surgery (score 0). Spearman correlation was performed between imaging and surgical PCI at the patient level. ROC analysis was performed at the patient level to determine diagnostic accuracy of DWI, CE-T1W, PET, and PET/MRI for diagnosing significant PC (PCI >20), a relative contraindication to CRS and HIPEC.
Results
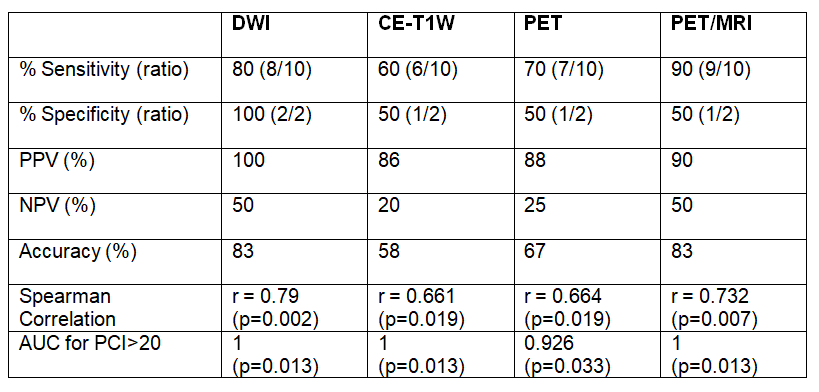
10/12 patients and 29/48 regions had surgically confirmed PC. Mean surgical PCI was 9.2±8.7 (range 0-24). Mean radiological PCI for DWI 6.7±9 (range 0-26), CE-T1W 6.3±7.1 (range 0-20), PET 3±3.5 (range 0-12), and PET/MRI 9.6±9 (range 0-27). Sensitivities and specificities at the patient and region level are listed in Figures 4 and 5. At the patient level, DWI demonstrated the highest individual modality sensitivity and specificity at 80% and 100%. Combined PET/MRI increased sensitivity to 90%, with a decrease in specificity to 50%. At the region level, DWI again demonstrated the highest sensitivity and specificity at 66% and 90%. PET had the lowest per region sensitivity at 38%. Combined PET/MRI increased sensitivity to 79%, but decreased specificity to 58%. Radiological PCI using DWI, CE-T1W, PET, and PET/MRI demonstrated significant correlation with surgical PCI: 0.790, 0.661, 0.664, and 0.732, respectively (p<0.019). DWI, CE-T1W, and PET/MRI all demonstrated perfect diagnostic performance for detection of PCI>20 (AUC=1, p=0.013).Discussion and Conclusion
PET/MRI was able to accurately score PCI at the patient level, but not at the region level. Combined PET/MRI increased sensitivity for the detection of PC, but with lower specificity. Previous studies have reported PC detection sensitivity and specificity at site level of DWI-MRI to be 74% and 97% and PET/CT to be 63% and 90%.4 Our combined PET/MRI data had better sensitivity than these reported values, but lower specificity. DWI, CE-T1W, PET, and PET/MRI demonstrated excellent diagnostic performance for detection of PCI>20, suggesting that PET/MRI may not necessarily be needed for diagnosing large tumor burden. Limitations of our study include using single readers for each imaging modality and small sample size. The utility of this hybrid imaging modality for PC detection and localization needs to be tested in a larger cohort of patients.Acknowledgements
None.References
- Spiliotis J, Halkia E, De bree E. Treatment of peritoneal surface malignancies with hyperthermic intraperitoneal chemotherapy-current perspectives. Curr Oncol. 2016;23(3):e266-75.
- Harmon RL, Sugarbaker PH. Prognostic indicators in peritoneal carcinomatosis from gastrointestinal cancer. Int Semin Surg Oncol. 2005;2(1):3.
- Schmidt S, Meuli RA, Achtari C, Prior JO. Peritoneal carcinomatosis in primary ovarian cancer staging: comparison between MDCT, MRI, and 18F-FDG PET/CT. Clin Nucl Med. 2015;40(5):371-7.
- Soussan M, Des guetz G, Barrau V, et al. Comparison of FDG-PET/CT and MR with diffusion-weighted imaging for assessing peritoneal carcinomatosis from gastrointestinal malignancy. Eur Radiol. 2012;22(7):1479-87.
Figures