2316
The effect of sunitinib treatment assessed by intravital microscopy and DCE-MRI in pancreatic ductal adenocarcinoma xenografts1Oslo University Hospital, Oslo, Norway
Synopsis
The effect of sunitinib treatment was evaluated by DCE-MRI, intravital microscopy, and immunohistochemistry in pancreatic ductal adenocarcinoma (PDAC) xenografts growing in dorsal window chambers or intramuscularly in the hind leg of mice. Sunitinib selectively removed small-diameter vessels and increased blood flow velocity. The increased blood flow velocity was not sufficient to compensate for the loss of tumor vessels, and, consequently, sunitinib-treated PDAC xenografts showed increased fractions of hypoxic tissue. Ktrans derived by pharmacokinetic analysis of DCE-MRI data was sensitive to microvascular density and hypoxia in both untreated and sunitinib-treated PDAC xenografts.
INTRODUCTION
Pancreatic ductal adenocarcinoma (PDAC) is an aggressive disease associated with poor outcome1. The low survival rates are primarily due to resistance to treatment which has been associated with poor blood supply and extensive hypoxia. Antiangiogenic treatment has been demonstrated to normalize tumor vasculature, improve perfusion, and increase tumor oxygenation in some preclinical studies, and to reduce blood supply and induce tumor hypoxia in others2,3. The reasons for these different effects are not well understood but may have substantial impact on combination therapies. Increased tumor oxygenation may improve the effect of ionizing radiation, immunotherapy, and some forms of chemotherapy, whereas elevated tumor hypoxia may impair the effects of the same treatment modalities4. The purpose of this study was to investigate whether sunitinib treatment can normalize the vasculature and increase oxygenation in PDAC xenografts, and to investigate whether DCE-MRI is sensitive to sunitinib-induced changes in these parameters.METHODS
BxPC-3 PDAC xenografts grown in dorsal window chambers or intramuscularly in the left hind leg of BALB/c nu/nu mice were used as tumor model. Tumor-bearing mice were treated with sunitinib (40 mg/kg/day for 4 days) or given vehicle, and were subjected to DCE-MRI, intravital microscopy, and histological examination. Parametric images of Ktrans and ve were derived from the DCE-MRI data by using Tofts pharmacokinetic model5. Morphologic parameters of tumor vascular networks were assessed from high-resolution transillumination images, and tumor blood supply times (BST) were assessed from first-pass imaging movies6. Microvascular density (MVD) and fraction of hypoxic tissue were assessed from immunohistochemical preparations by using CD31 and pimonidazole as markers of microvessels and hypoxia.RESULTS AND DISCUSSION
The dorsal window chamber preparation allowed daily assessment of the tumor vasculature (Figure 1). Sunitinib treatment reduced the density of small-diameter vessels but did not affect the density large-diameter vessels (Figure 1B). The selective removal of small-diameter vessels resulted in increased vessel diameter and increased vessel segment length (Figure 1B). Sunitinib-treated tumors showed reduced BST values, implying that the blood flow velocity was higher in the surviving vessels (Figure 2). The increased blood flow velocity was probably caused by the selective removal of small-diameter vessels. Small-diameter vessels are expected to have a high geometric resistance to blood flow because the geometric resistance in tubes with laminar flow is inversely proportional to the vessel diameter to the fourth power7. In intramuscular tumors, sunitinb treatment reduced MVD and increased the fraction of hypoxic tissue (Figure 3). Sunitinib treatment also reduced Ktrans values but did not affect ve values (Figure 4A-C). Strong correlations were found between Ktrans and MVD and between Ktrans and hypoxic fraction for both untreated and sunitinib-treated tumors (Figure 4D-E). When tumors with similar MVD were compared, sunitinib-treated tumors had higher Ktrans and lower hypoxic fraction than untreated tumors (Figure 3D and Figure 4D), suggesting that the surviving vessels in the treated tumors were more efficient.CONCLUSION
Sunitinib treatment selectively removed small-diameter vessels and increased blood flow velocity. The increased blood flow velocity could not compensate for the loss of tumor vessels, and, consequently, the sunitinib-treated BxPC-3 tumors showed increased hypoxic fractions. Ktrans derived from DCE-MRI data was sensitive to MVD and hypoxia in both untreated and sunitinib-treated tumors, and may be used to monitor the effect of sunitinib treatment in tumors similar to BxPC-3 tumors.Acknowledgements
No acknowledgement found.References
1 Garrido-Laguna I, Hidalgo M. Pancreatic cancer: from state-of-the-art treatments to promising novel therapies. Nat Rev Clin Oncol. 2015;12: 319-334.
2 Winkler F, Kozin SV, Tong RT, et al. Kinetics of vascular normalization by VEGFR2 blockade governs brain tumor response to radiation: role of oxygenation, angiopoietin-1, and matrix metalloproteinases. Cancer Cell. 2004;6:553-563.
3 Franco M, Man S, Chen L, et al. Targeted anti-vascular endothelial growth factor receptor-2 therapy leads to short-term and long-term impairment of vascular function and increase in tumor hypoxia. Cancer Res.2006;66:3639-3648.
4 Horsman MR, Siemann DW. Pathophysiologic effects of vascular-targeting agents and the implications for combination with conventional therapies. Cancer Res. 2006;66:11520-11539.
5 Gaustad JV, Simonsen TG, Smistad R,. et al. Early effects of low dose bevacizumab treatment assessed by magnetic resonance imaging. BMC cancer. 2015;15:900.
6 Øye KS, Gulati G, Graff BA, et al. A novel method for mapping the heterogeneity in blood supply to normal and malignant tissues in the mouse dorsal window chamber. Microvasc Res. 2008;75:179-187. 7 Jain, R. K. Determinants of tumor blood flow: a review. Cancer Res.1988;48:2641-2658.
Figures
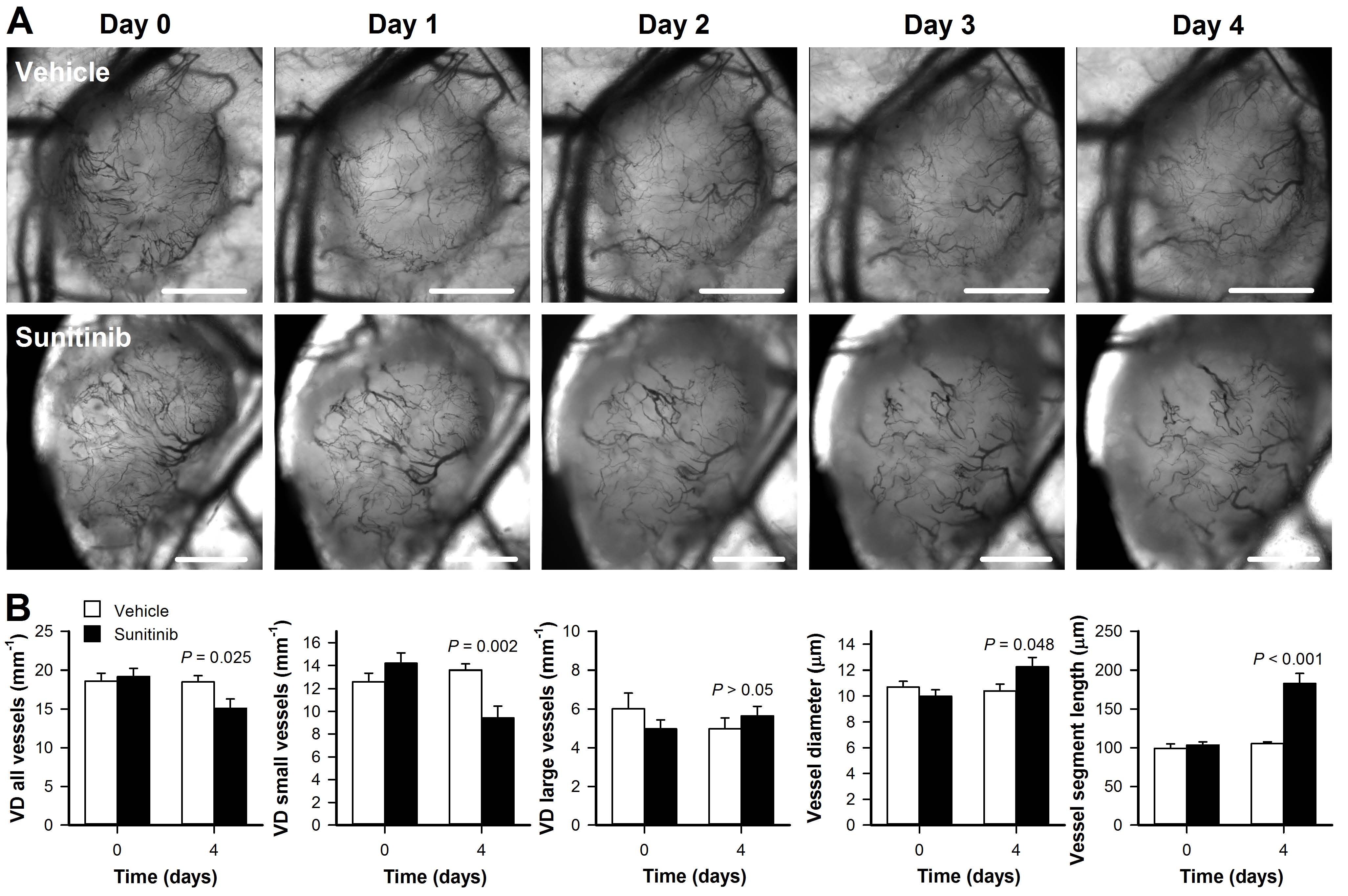
Figure 1. Sunitinib treatment selectively removed small-diameter vessels.
A, Daily intravital microscopy images of an untreated (upper row) and a sunitinib-treated BxPC-3 tumor recorded before (day 0) and throughout the treatment period (day 1-4). Scale bars, 1mm. B, Vessel density (VD) of all vessels, VD of small-diameter vessels (<15μm), VD of large-diameter vessels (>15μm), vessel diameter, and vessel segment length in untreated and sunitinib-treated BxPC-3 tumors before (day 0) and after treatment (day 4). Columns, means of 7 tumors; bars, SEM.
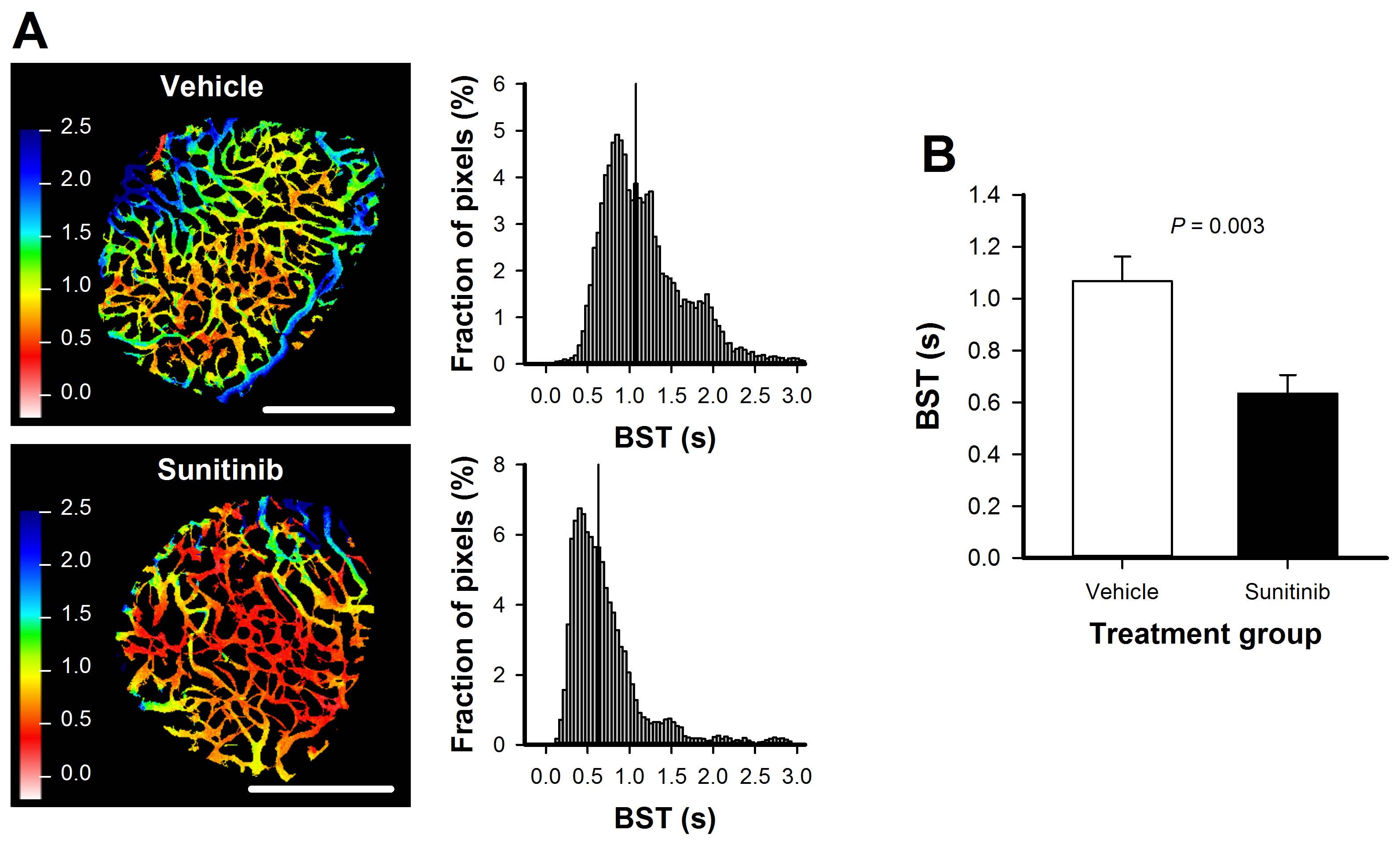
Figure 2. Sunitinib treatment reduced blood supply time.
A, Blood supply time (BST) image and BST frequency histogram of an untreated and a sunitinib-treated BxPC-3 tumor. BST images were produced from first-pass imaging movies recorded after an intravenous bolus injection of fluorescence-labeled dextran. Color bars, BST scales in seconds; scale bars, 1mm. B, BST in untreated and sunitinib-treated BxPC-3 tumors. Columns, means of 6 tumors; bars, SEM.
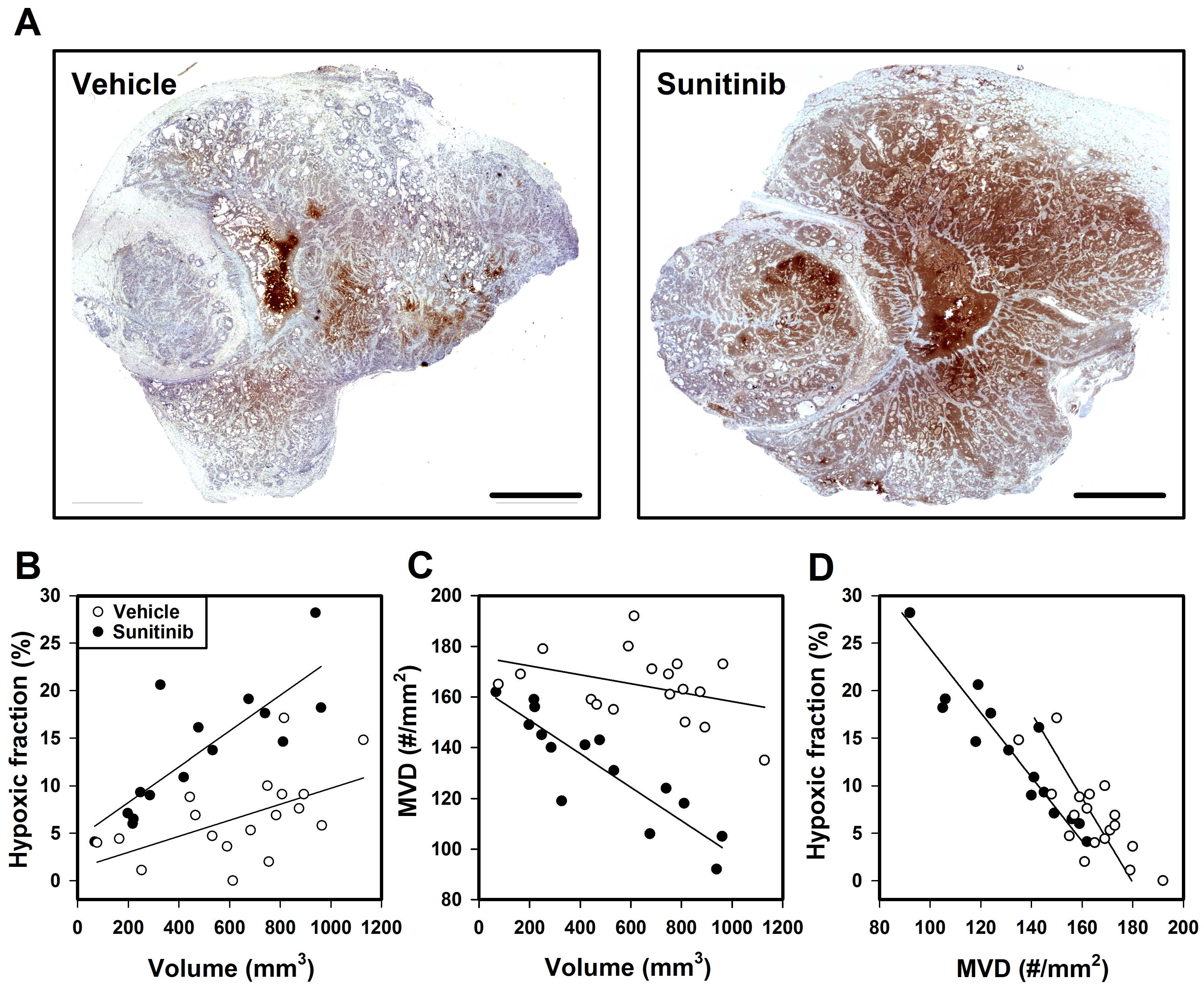
Figure 3. Sunitinib treatment induced tumor hypoxia.
A, Histological preparations stained for pimonidazole to visualize regions with hypoxic tissue in an untreated and a sunitinib-treated BxPC-3 tumor. Scale bars, 2mm. B-D, Fraction of hypoxic tissue versus tumor volume, microvascular density (MVD) versus tumor volume, and fraction of hypoxic tissue versus MVD for untreated and sunitinib-treated BxPC-3 tumors. Points, individual tumors; curves, linear regression fits.
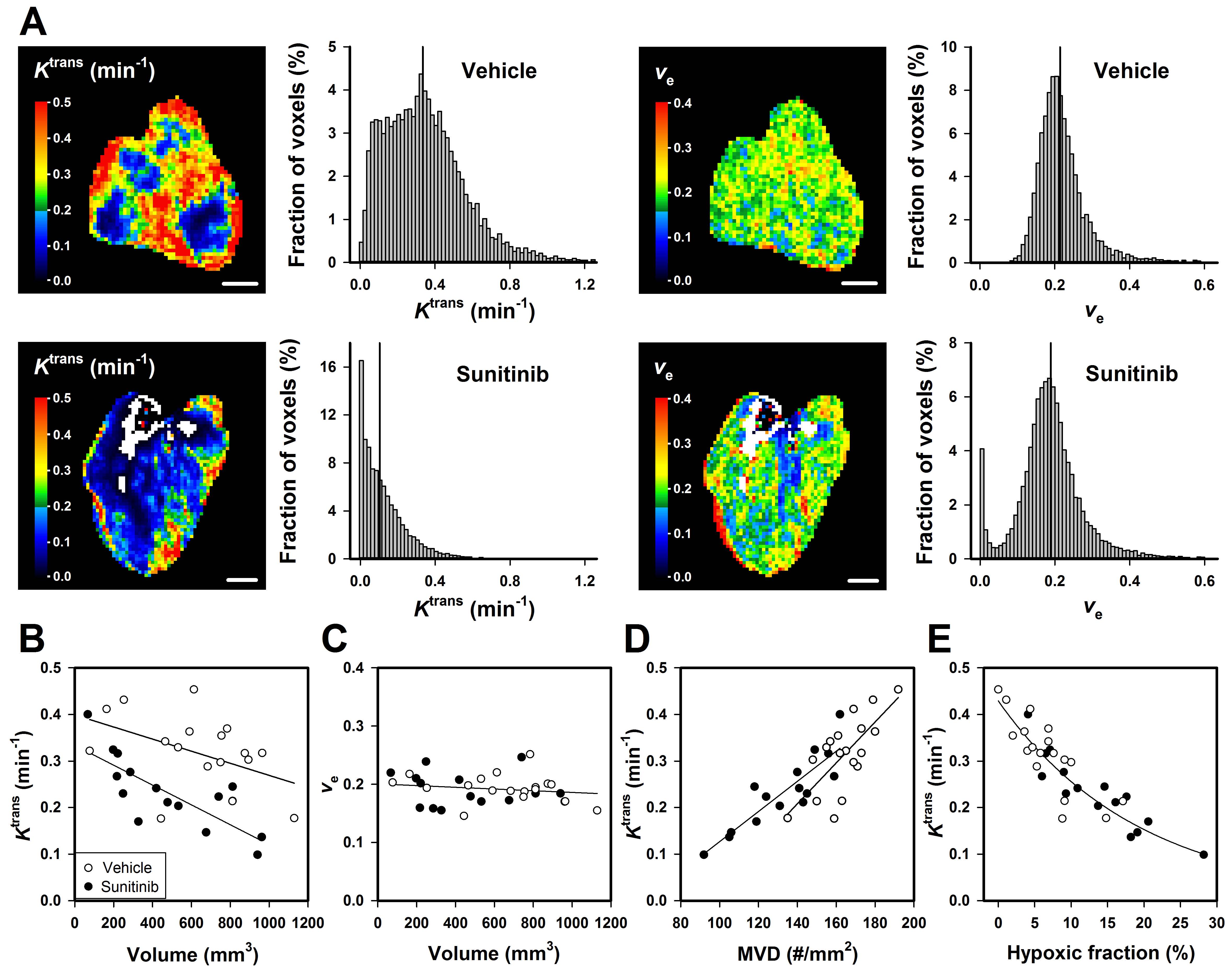
Figure 4. DCE-MRI was sensitive to sunitinib-induced changes in the tumor microenvironment.
A, Ktrans and ve images and frequency distributions of an untreated and a sunitinib-treated BxPC-3 tumor. Color bars, Ktrans or ve scales; scale bars, 2mm. B-E, Ktrans versus tumor volume, ve versus tumor volume, Ktrans versus microvascular density (MVD), and Ktrans versus fraction of hypoxic tissue for untreated and sunitinib-treated BxPC-3 tumors. Points, individual tumors; curves, linear or exponential regression fits. A single curve was fitted to the data when the data for untreated and sunitinib-treated tumors were not significantly different.