2308
Comparison of the Capability for Quantitative Distinguishing Malignant from Benign Solitary Pulmonary Nodules among actual DWI, computed DWIs with different b values and FDG-PET/CT1Division of Radiology, Department of Radiology, Kobe University Graduate School of Medicine, Kobe, Japan, 2Canon Medical Systems Corporation, Otawara, Japan, 3Division of Functional and Diagnostic Imaging Research, Department of Radiology, Kobe University Graduate School of Medicine, Kobe, Japan, 4Advanced Biomedical Imaging Research Center, Kobe University Graduate School of Medicine, Kobe, Japan, 5Center for Radiology and Radiation Oncology, Kobe University Hospital, Kobe, Japan
Synopsis
There are no major papers that compared differentiating capability of SPNs among actual DWI (aDWI), computed DWIs (cDWIs)with different b values and FDG-PET/CT in patients with SPN. We hypothesize that cDWI obtained appropriate b value can improve the capability for differentiating malignant from benign SPNs as compared with aDWI and FDG-PET/CT. The purpose of this study is to directly compare the capability for differentiating malignant from benign pulmonary nodules among aDWI, cDWIs with different b values and FDG-PET/CT.
Introduction
Solitary pulmonary nodule (SPN) is a common radiological finding, and its’ differentiation is one of the important clinical questions in routine clinical practice. Many different approaches by computed tomography (CT) and positron emission tomography fused with CT (PET/CT) combined with [18F] fluoro-2-D-glucose (FDG) have been tested in the last a few decades. Magnetic resonance imaging (MRI) has been also applied for chest diseases since late 1990s and demonstrated its’ clinical relevance in the last a few decades. In the last a few decades, short-TI inversion recovery (STIR) turbo spin-echo imaging, diffusion weighted imaging (DWI), and dynamic contrast-enhanced MRI have been reported as useful in this setting (1-3). Recently, computed DWI (cDWI) generated from actually obtained DWI (aDWI) at two different b values has been reported as useful for improving image quality and improving diagnostic performance in prostatic cancer patient. (4, 5). However, there are no major papers that compared differentiating capability of SPNs among aDWI, cDWIs with different b values and FDG-PET/CT in patients with SPN. We hypothesize that cDWI obtained appropriate b value can improve the capability for differentiating malignant from benign SPNs as compared with aDWI and FDG-PET/CT. The purpose of this study is to directly compare the capability for differentiating malignant from benign pulmonary nodules among aDWI, cDWIs with different b values and FDG-PET/CT.Materials and Methods
65 consecutive patients (44 men and 21 women; mean age ± standard deviation, 69.5±8.7) with 85 pulmonary nodules prospectively underwent aDWI at a 3T MR system (Vantage Titan 3T, Canon Medical Systems Corporation), integrated FDG-PET/CT, pathological, microbacterial and follow-up examinations. According to results of pathological and follow-up examinations, all nodules were divided into malignant (n=48) and benign (n=37) nodule groups. In each patient, aDWI was obtained by fast advanced spin-echo sequence (TR, 13,500-16,000 ms; TE, 70-90 ms; ETL, 36-40; b value = 0 and 1000 s/mm2) with the spectral attenuated inversion recovery technique under free breathing. All cDWIs were generated by a commercially available software (M-Power, Canon Medical Systems) in each patient. In this study, cDWIs were computationally generated as DWIs at 600s/mm2 (cDWI600), 800s/mm2 (cDWI800) and 1500s/mm2 (cDWI1500) from aDWIs at 0 and 1000 s/mm2 (aDWI1000). Then, ROI was placed over each nodule on all images for evaluating signal intensity (SI) and SUVmax without any information for final diagnosis. To normalize SIs at all SPNs on each DWI, contrast ratios (CRs) between SPN and thoracic muscle were calculated.
To compare all indexes between malignant and benign groups, Student’s t-test was performed. To compare differentiation capability of pulmonary nodule among all methods and determine each threshold value, ROC analyses were performed. Then, sensitivity, specificity and accuracy were compared among all each other by McNemar’s test. A p value < 0.05 was considered statistically significant in this study.
Results
Representative cases are shown in Figure 1 and 2. There was significant difference of each index between malignant and benign SPN groups (p<0.05). Results of ROC analysis are shown in Figure 3. Area under the curve (AUC) of cDWI600 (AUC=0.92) was significantly larger than that of SUVmax (AUC=0.82, p=0.02). Results of compared diagnostic performance among all methods are shown in Figure 4. Sensitivity of SUVmax was significantly lower than that of each cDWI and aDWI1000 (p<0.05). In addition, sensitivities of aDWI1000 and cDWI1500 were significantly lower than that of cDWI600 (p<0.05). Accuracy of SUVmax was significantly lower than that of aDWI1000, cDWI600 and cDWI800 (p<0.05). Moreover, accuracies of aDWI1000 and cDWI1500 were significantly lower than that of cDWI600 (p<0.05).Conclusion
Computed and actual DWIs have a better potential for differentiating malignant from benign SPNs than FDG-PET/CT. In addition, computed DWI would be better to be generated at b value as 600s/mm2 for improving diagnostic performance of DWI in this setting.Acknowledgements
No acknowledgement found.References
1. Koyama H, Ohno Y, Kono A, et al. Eur Radiol. 2008; 18: 2120-2131.
2. Ohno Y, Koyama H, Takenaka D, et al. J Magn Reson Imaging. 2008; 27: 1284-1295.
3. Koyama H, Ohno Y, Seki S, et al. Eur J Radiol. 2015; 84: 509-515.
4. Blackledge M.D, Leach M.O., Collins D.J., et al. Radiology 2011:261;573-581.
5. Ueno Y, Takahashi S, Kitajima K, et al. Eur. Radiol., 2013;23:3509-3516.
Figures

Figure 1. 48-year old male with adenocarcinoma with lipidemic pattern in the left upper lobe.
CRs of aDWI1000 and cDWIs and SUVmax were determined as follows: aDWI1000, 6.4; cDWI600, 6.4; cDWI800, 6.4; cDWI1500, 6.1; and SUVmax, 6.1. With applying each threshold value, all methods could accurately diagnose this case as malignant.

Figure 2. 70-year old male with invasive adenocarcinoma in the right upper lobe.
CRs of aDWI1000 and cDWIs and SUVmax were determined as follows: aDWI1000, 1.5; cDWI600, 3.4; cDWI800, 1.5; cDWI1500, 1.3; and SUVmax, 1.1. With applying each threshold value, all methods except cDWI600 could not accurately diagnose this case as malignant.
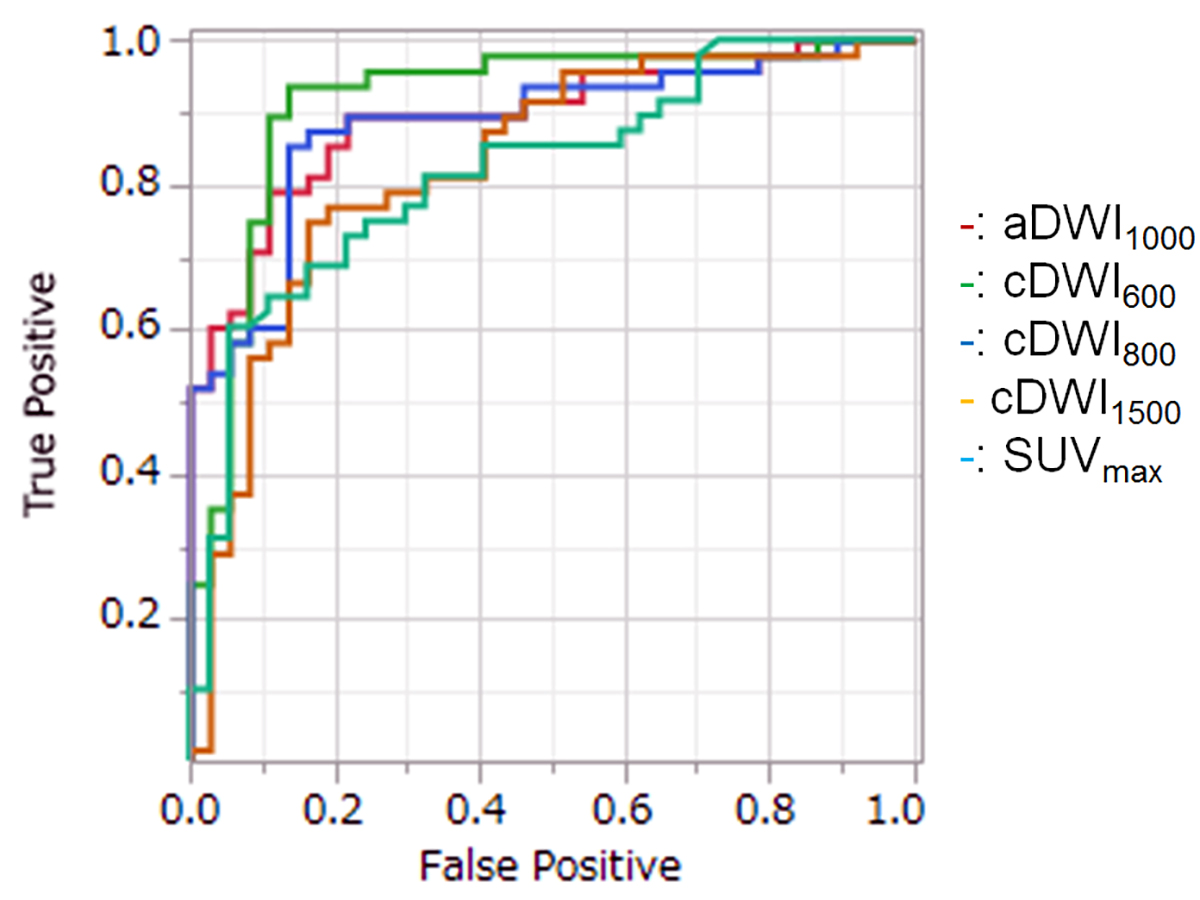
Figure 3. Results of ROC analysis among all indexes.
Area under the curve (AUC) of cDWI600 (AUC=0.92) was significantly larger than that of SUVmax (AUC=0.82, p=0.02).
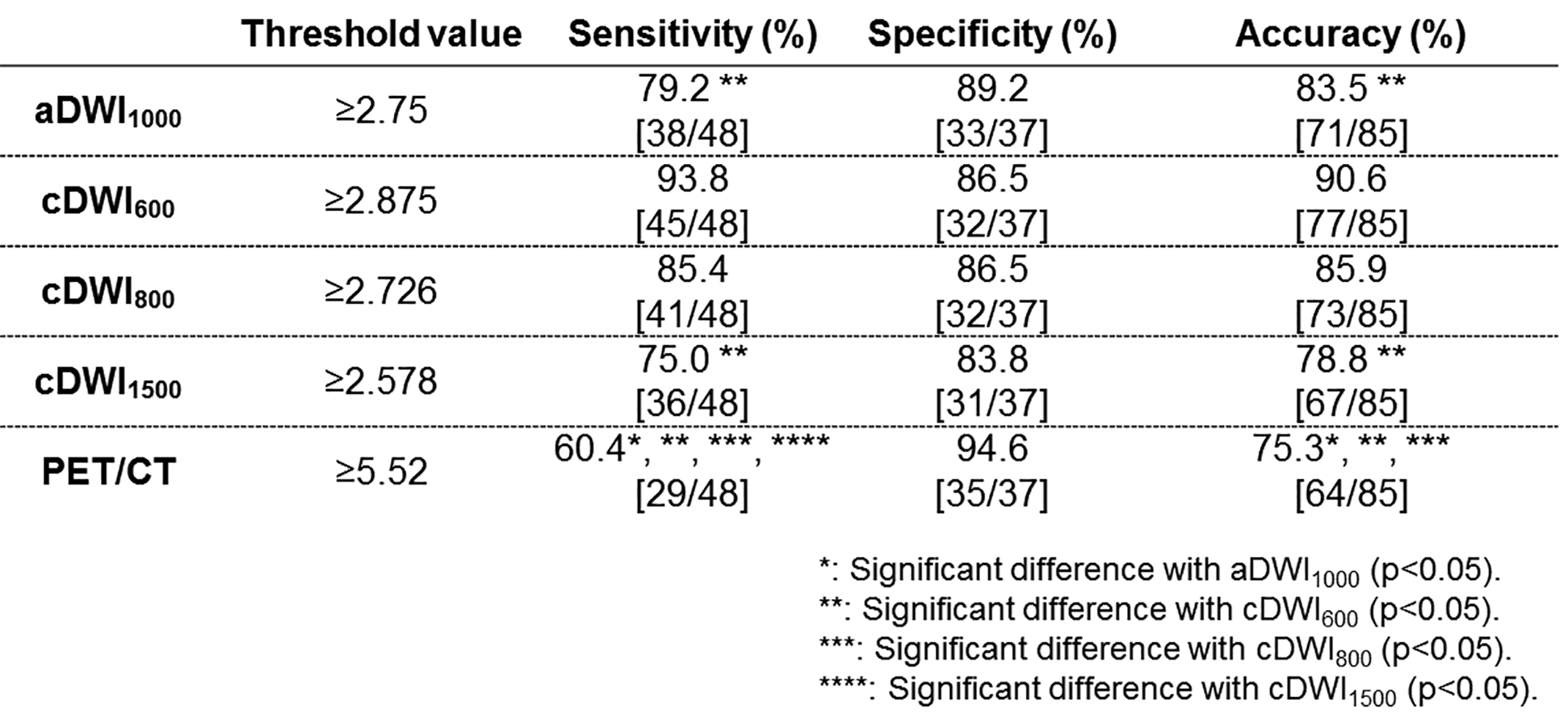
Figure 4. Comparison of diagnosic performance among all indexes.
Sensitivity of SUVmax was significantly lower than that of each cDWI and aDWI1000 (p<0.05). Moreover, sensitivities of aDWI1000 and cDWI1500 were significantly lower than that of cDWI600 (p<0.05). Accuracy of SUVmax was significantly lower than that of aDWI1000, cDWI600 and cDWI800 (p<0.05). In addition, accuracies of aDWI1000 and cDWI1500 were significantly lower than that of cDWI600 (p<0.05).