2302
Design and validation of an MRI-based oxygen sensor for a cervical cancer clinical trial1Koch Institute for Integrative Cancer Research, Massachusetts Institute of Technology, Cambridge, MA, United States, 2Department of Radiology, Brigham and Women's Hospital, Boston, MA, United States, 3Department of Radiation Oncology, Brigham and Women's Hospital, Boston, MA, United States, 4Department of Materials Science and Engineering, Massachusetts Institute of Technology, Cambridge, MA, United States
Synopsis
Many cancer patients experience lower survival rates if they have less well oxygenated tumors. Lower tumor oxygen levels can lead to a reduced effectiveness of radiation therapy. The ability to overcome this radiotherapy resistance has been severely limited by the lack of a clinically compatible quantitative oxygen sensing technology. We report the design and validation of a silicone-based oxygen sensor measured with MRI for an approved human clinical trial in patients with cervical cancer. The sensor has been validated for compatibility with the clinical workflow and is specifically designed to achieve the endpoints of the trial.
Introduction
Hypoxia, the extreme depletion of tissue oxygen, is a hallmark of solid tumors and has been linked to chemo- and radiotherapy-resistance and a generally poor prognosis for patients. This has been observed in many cancers including cervical,1 prostate,2 and head and neck.3 A compelling treatment approach is the delivery of an increased radiation dose to hypoxic tumor sub-volumes. High dose-rate brachytherapy (HDR-brachy) is the most effective option to achieve dose escalation in hypoxic regions of a tumor without exposing healthy tissue and organs to unsafe radiation levels. Tumor oxygen levels are not currently considered during the standard treatment and dose planning processes. Attempts to overcome hypoxia have been of limited clinical utility due to the lack of an appropriate oxygen measurement technique to quantitatively map tumor hypoxia. The Cima Lab has developed a silicone-based quantitative oxygen sensor that is measured with MRI.4 We report on the development and implementation of an embodiment of the silicone oxygen sensor for an early feasibility human clinical trial in ten patients with locally advanced cervical cancer. The focus of the presented work is on the transition of the silicone sensor to a clinical MRI and validation of the new sensor embodiment to ensure that it meets the necessary requirements for our upcoming human clinical trial.
The oxygen sensor catheter will be evaluated during the MRI-guided placement of HDR-brachy treatment catheters. This study will evaluate the temporary insertion, measurement, and removal of two oxygen sensors. This early feasibility study will be used to measure oxygen levels in a solid tumor and inform design decisions for subsequent versions of the sensor, but will not be used to make modifications to treatment. The effectiveness of modifying treatment based on oxygen measurements using this family of materials will be evaluated in a future clinical trial.
Methods
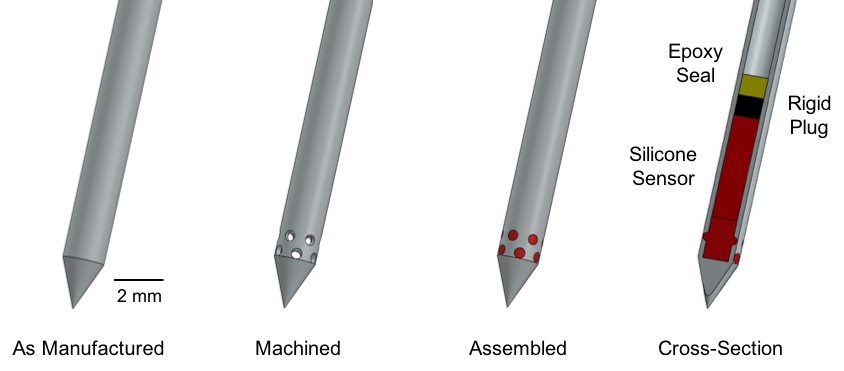
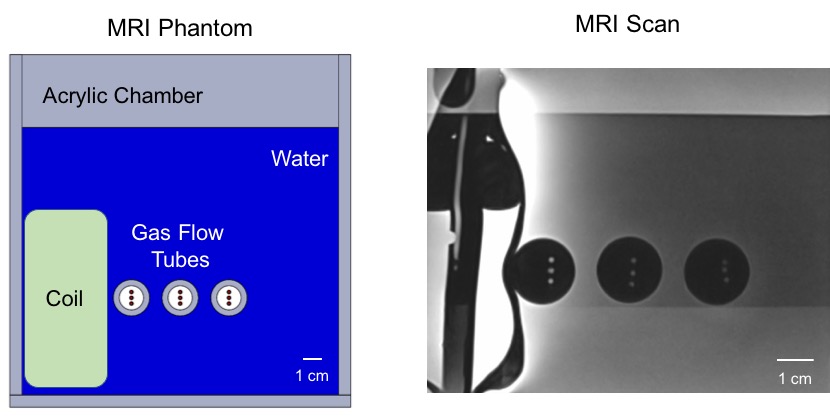
Standard brachytherapy treatment catheters were modified by machining the tip to add twelve holes (0.51 mm diameter) for oxygen exchange (Figure 1). The tip of the brachytherapy treatment catheter was then filled with the quantitative silicone oxygen sensor. A range of silicone sensor formulations was evaluated for sensitivity using a 0.5 T benchtop relaxometer (Bruker Minispec). Validation of the oxygen sensor catheters was conducted in an MRI-compatible environmental test chamber (Figure 2) that allows the concentration of oxygen to be modified during data collection. The test chamber also positions an endorectal receive coil in close proximity (1 to 6 cm) to the oxygen sensor catheters to mimic their relative positioning during the clinical trial. All catheter measurements were made using a 3 T MRI scanner (Siemens Verio) with endorectal, spine, and body matrix receive coils. T1 (spin-lattice) relaxation measurements are conducted using an inversion recovery turbo spin echo sequence. MRI data acquisition was conducted using the following parameters, inversion range: 24 to 2800 ms, repetition time: 3000 ms, echo time: 15 ms, slice thickness: 2 mm, matrix: 260 x 320, and field of view: 97 x 120 mm.Results
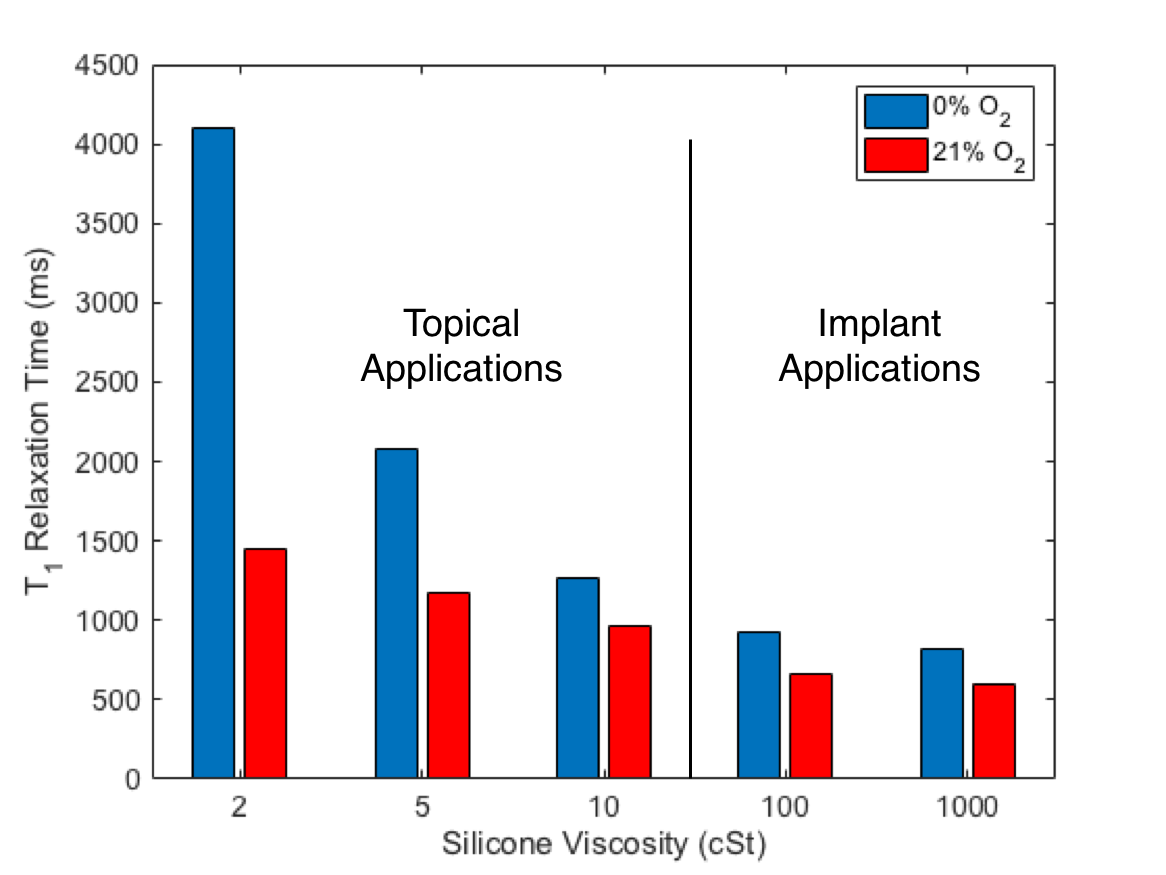
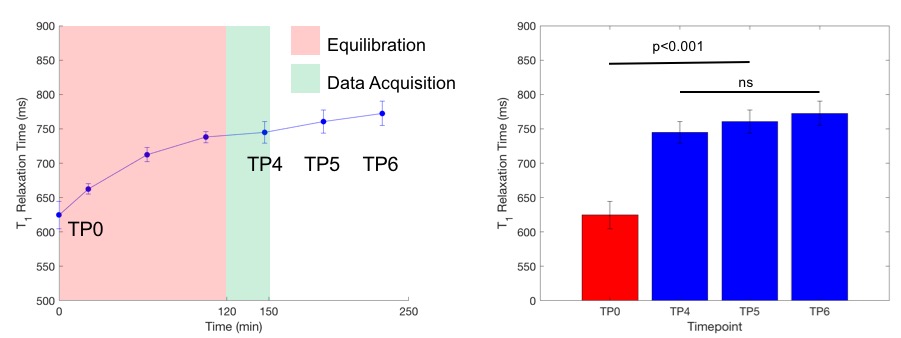
A design decision was made to choose a silicone formulation that utilized materials already intended for implantable use. Based on this criteria, a 100 cSt silicone sensor formulation was selected, as it offered the greatest sensitivity of available implant-grade materials (Figure 3). MRI performance of the oxygen sensor catheter was validated for sensitivity and equilibration time. Catheters were determined to equilibrate within 120 minutes following initial exposure to a 0% oxygen environment (Figure 4) and the sensor is capable of distinguishing between poorly (0%) and well (21%) oxygenated environments as required for this study.Discussion
The design implemented for the early feasibility trial is appropriate and capable of collecting the endpoints of our upcoming clinical trial. These results will provide quantitative information of solid tumor oxygen content, validate our proposed methodology for integrating oxygen sensing into the clinical workflow, and inform subsequent design decisions for future generations of the oxygen sensor. This study imposed specific constraints including the use of materials already designated for implantable use. This specific constraint will be relaxed moving forward, and formulations with higher sensitivity silicones will be validated for functional performance and biocompatibility and implemented for clinical use.Conclusion
Silicone-based oxygen sensors are a viable method of quantifying tumor oxygen content using clinical MRI hardware and pulse sequences. Implementation of this sensor for this clinical trial will provide the necessary information to successfully guide the development of this family of sensors for clinical use.Acknowledgements
This work is supported by the Bridge Project Expansion Grant (Koch Institute for Integrative Cancer Research/Dana-Farber) and the Image Guided Therapy Center (NIH P41EB015898). G. Ekchian is currently supported by the Koch Institute Quinquennial Cancer Research Fellowship.References
1 Hockel, M. et al. Association between tumor hypoxia and malignant progression in advanced cancer of the uterine cervix. Cancer Res 56, 4509-4515 (1996).
2 Milosevic, M. et al. Tumor Hypoxia Predicts Biochemical Failure Following Radiotherapy for Clinically Localized Prostate Cancer. Clinical Cancer Research (2012).
3 Janssen, H. et al. Hypoxia in head and neck cancer: how much, how important? Head Neck 27, 622-638, doi:10.1002/hed.20223 (2005).
4 Liu, V. et al. Solid MRI contrast agents for long-term, quantitative in vivo oxygen sensing. Proc Natl Acad Sci U S A 111, 6588-6593, doi:10.1073/pnas.1400015111 (2014).
Figures