2299
Magnetic Resonance Imaging of Oxygen Carriers in Treatment of Hypoxic Tumours1Institute of Biomedical Engineering, University of Oxford, Oxford, United Kingdom, 2University of Nottingham, Nottingham, United Kingdom, 3Department of Oncology, University of Oxford, Oxford, United Kingdom
Synopsis
It is established that tumour hypoxia is a predictor of cancer disease progression, treatment failures, and metastatic potential. There remains a need for oxygen delivery mechanisms for hypoxia reduction. The ideal method for measuring oxygen in tissue is noninvasive and quantitative, allowing tumour pO2 measurements to be obtained before, during, and after treatment. We investigated effects of oxygen nano-carriers on the longitudinal relaxation times of tumour tissues in vivo and a phantom. T1 decreased with increased oxygen concentration in phantom. The injection of the oxygenated nanobubbles resulted in a statistically significant decrease in T1-weighted signal when measured 6-8 minutes post-injection.
Introduction
It is well established that tumour hypoxia is a predictor of disease progression, treatment failures, and metastatic potential. To date, methods for reducing tumour hypoxia have delivered limited success owing to either a lack of proven efficacy, unwanted side effects, or logistical limitations. Therefore, there remains an urgent requirement for an effective hypoxia reduction mechanism that is safe, cost effective, biocompatible, and easy to use. To address this, oxygen-filled micro and nanobubbles have been investigated as a method of oxygen delivery and have shown promising results at improving therapy response. To continue effective research of oxygen carriers and hypoxia reduction, consistent methods for measuring oxygen release should be established. The ideal method for measuring oxygen in tissue would be noninvasive and quantitative, allowing tumour pO2 measurements to be obtained before, during, and after treatment. As MRI is a widely clinically available, non-ionizing, non-invasive imaging technique, it is ideal for determining tissue oxygenation noninvasively. Several MRI studies have examined oxygenation by observing the effect of oxygen on T1 shortening [1,2]. The effect of oxygen concentration on longitudinal relaxation is varied among various tissues [2], and the effect of oxygen carriers on the longitudinal relaxation of hypoxic tumour tissues has yet to be examined. In this project, we investigated the effects of these oxygen nano-carriers on the longitudinal relaxation times of tumour tissues in vivo and in a phantom using MRI.Methods
For the in vivo experiments, two C57 mice bearing subcutaneous pancreatic cancer B8484 tumours were used as a model for human pancreatic cancer. Oxygenated nanobubbles (O2NBs) were administered via a tail-vein injection. A T1-weighted MRI (TR = 1.6ms, TE = 0.656ms) was collected every 12 seconds for 50 timepoints resulting in 10 minutes total. The injection began 72 seconds into the scan time and was complete after 25 seconds. The imaging experiments were performed using a 7.0 tesla 210mm horizontal bore VNMRS preclinical imaging system equipped with 12mm bore gradient insert (Varian Inc. Palo Alto, CA, USA).
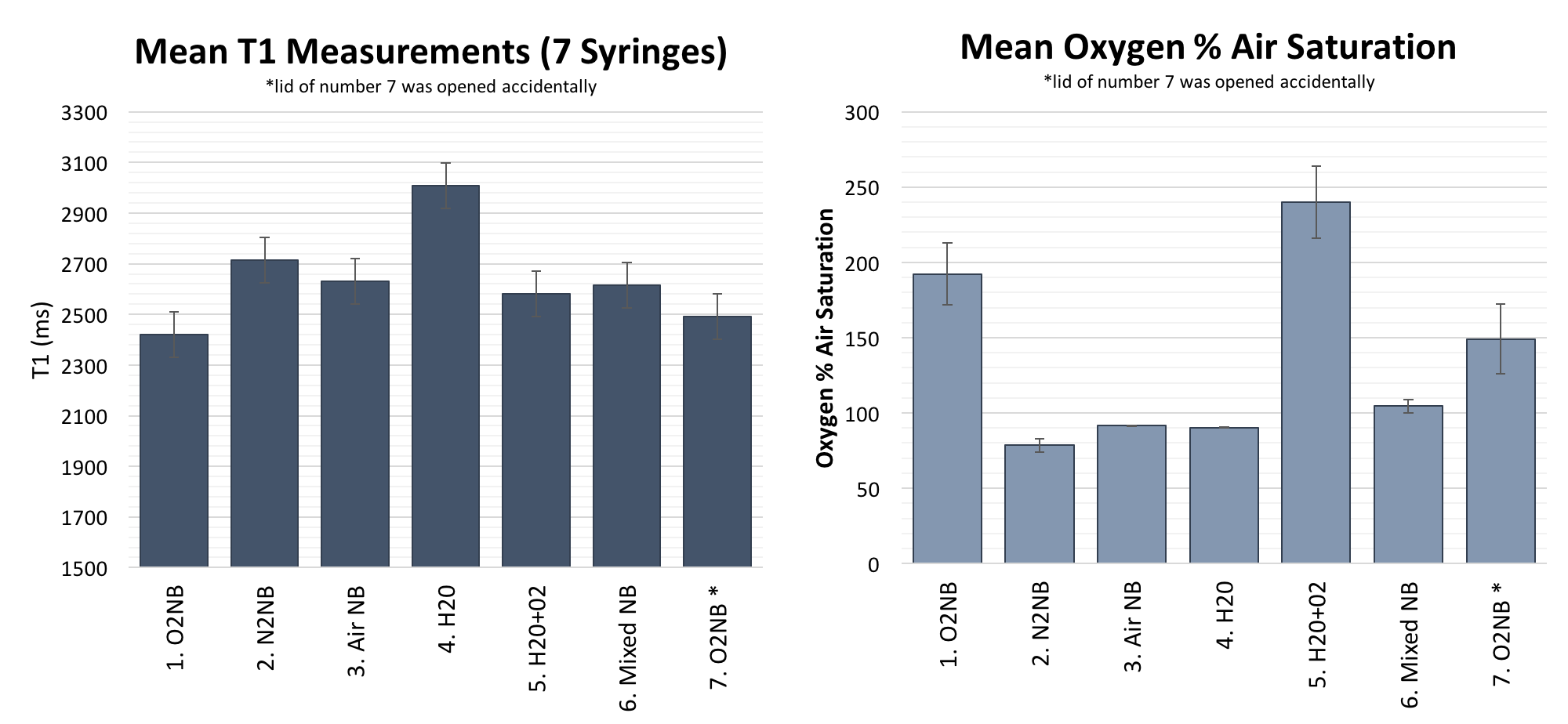
For the phantom experiments, to measure the T1 of solutions with varying oxygen content, seven different solutions were prepared: O2NB, N2NB, air NB, water, oxygenated water, half O2NB and half N2NB mixture, and a second O2NB solution. For these phantom experiments, VFA MRI were acquired with a 3D gradient echo sequence (TR = 3.2ms, TE = 0.664ms, FA = 1, 1.2, 1.4, 1.6, 1.8, 2, 2.2, 2.4, 2.7, 3.1, 3.7, 4.4, 5.2, 6.1, 7, 8). The nanobubble (NB) solutions were prepared according to Owen et al [3]. To create 100ml of the nanobubble solution, glycyrrhizic acid (0.5mg/ml), lecithin (3 mg/ml), citric acid (5 mg/ml) and glycerol (0.0125 ml/ml) were mixed with 100ml of boiled, filtered de-ionized water. The solution was stirred for 30 minutes. Next, 5 ml of the solution was transferred to a glass vial and sparged with either O2 gas, N2 gas, or air for 3 minutes, sealed and mechanically agitated for 30s. To produce oxygenated water, filtered deionized water was sparged with O2 gas for 3 minutes.
Results & Discussion
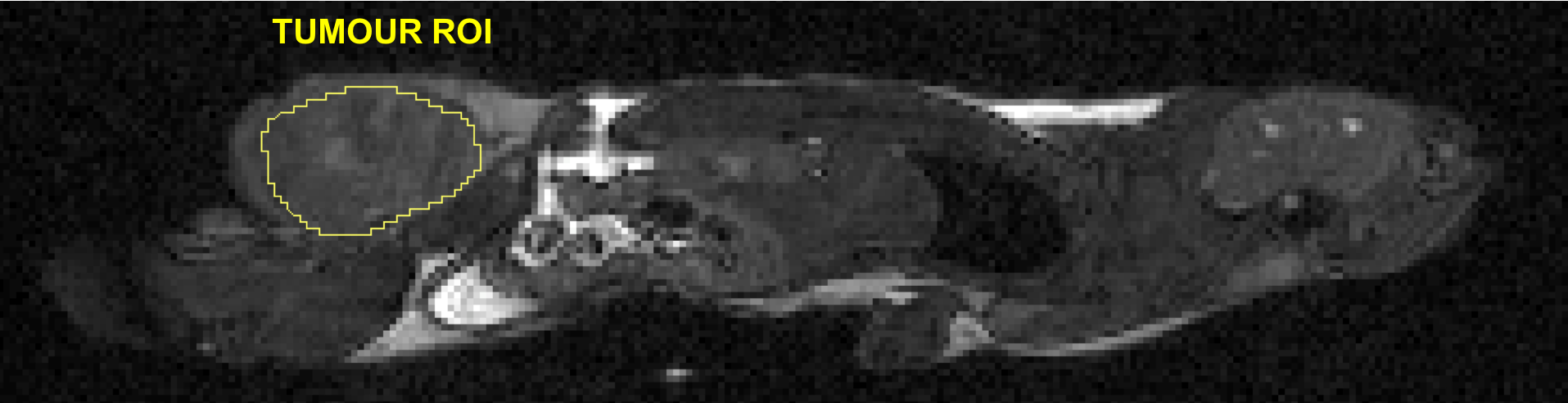
These experiments served as a pilot to study the effects of these oxygen nano-carriers on the longitudinal relaxation times of tumour tissues in vivo and in a phantom. The relationships between the T1 values and oxygen concentration from the phantom experiment (shown in Figure 2) were proportionally consistent with previous findings from our laboratory and showed a shortened longitudinal relaxation time with increased oxygen. However, the injection of the O2NBs resulted in a statistically significant decrease (p=0.046) in T1-weighted signal intensity of the tumour region when measured 6-8 minutes post-injection. An example slice of the 3D region of interest selected is in Figure 3. In contrast, no significant change in T1 was observed in the brain and fat tissues (p=0.8 and p=0.4, respectively). Based on theory and phantom results, an increase in T1-weighted signal intensity would have been expected, and it is likely that 10 minutes was not long enough to appropriately measure the change in oxygenation caused by the nanobubbles. It is not possible to conclude results from this single mouse pilot study, and the results have been helpful in designing the follow-up study with a larger sample size and quantitative VFA T1 maps being collected at 5 minute time points for 30 minutes following injection. Ultimately, the ability to quantify T1 changes during oxygen delivery and relate them to anti-cancer therapy outcomes is the objective of this research.Acknowledgements
This work was supported by funding from the Clarendon Scholarship and the Engineering and Physical Sciences Research Council (EPSRC) and Medical Research Council (MRC) [grant number EP/L016052/1] and Programme Grant (EP/L024012/1): Oxford Centre for Drug Delivery Devices, the Cancer Research UK Pioneer Award: Oral formulation of oxygen for tumour hypoxia, the Institute of Engineering & Technology: AF Harvey Prize.References
- Berkowitz BA. Role of dissolved plasma oxygen in hyperoxia induced contrast. Magn Reson Imaging (1997).
- Tadamura, E., Hatabu, H., Li, W., Prasad, P. V. & Edelman, R. R. Effect of oxygen inhalation on relaxation times in various tissues. Magn Reson Imaging (1997).
- Owen, J. et al. Reducing Tumour Hypoxia via Oral Administration of Oxygen Nanobubbles. PLoS ONE (2016).
Figures