2281
Comparison of LCModel fitting of HRMAS spectra acquired from malignant glioma tissue using free induction decay and Carr-Purcell-Meiboom-Gill pulse sequences1Department of Radiology & Imaging Sciences, Emory University School of Medicine, Atlanta, GA, United States
Synopsis
Gliomas are a class of aggressive brain tumors with a low survival rate. New biomarkers are needed to monitor tumor progression and response to treatment. Our goal was to compare the effectiveness of operator-independent LCModel analysis for HRMAS NMR spectra acquired from histologically confirmed glioma tissue (n=14) using both FID and CPMG pulse sequences. The CRLBs of lactate and myo-inositol were significantly lower for spectra acquired with the CPMG compared to the FID sequence. Relevant glioma metabolites were quantified with LCModel from most spectra acquired with CPMG but not FID.
Introduction
Gliomas are a class of aggressive brain tumors with a median survival rate of 12-15 months and a five-year survival rate of less than 5% in its most aggressive form.1,2 Given high rates of treatment resistance and low survival rates, new imaging biomarkers to monitor tumor progression and characterize response to treatment are necessary.
High-resolution magic angle spinning (HRMAS) nuclear magnetic resonance (NMR) spectroscopy is a tool that can identify and quantify metabolite concentrations in glioma tissue. While this experimental method has been previously validated, most analysis is performed with software that requires manual peak selection and integration that can prevent accurate and reliable quantification of overlapping peaks and large macromolecule baselines. Our goal was to compare the effectiveness of operator-independent LCModel analysis of glioma spectra acquired from free induction decay (FID) and Carr-Purcell-Meiboom-Gill (CPMG) sequences.
Methods
HRMAS solid-state NMR spectra were acquired from 14 histologically-confirmed glioma samples (WHO grades II (n=5), III (n=5), and IV (n=4)) collected during surgical resection from human brain tumor patients. 10-15 mg of frozen tissue was extracted using a biopsy punch and placed in an 80 μL disposable MAS insert (Bruker) inside a 4 mm zirconium MAS rotor. Spectra were acquired at 4 ⁰C using a 600 MHz Bruker NMR spectrometer with both FID and CPMG pulse sequences with a pre-saturation water suppression pulse and the following parameters: MAS spinning speed: 4 kHz; complex data points = 16384; bandwidth = 8013 Hz; n=512. Brain metabolite concentration ratios and Cramer-Rao lower bounds (CRLBs) of the metabolites were estimated using LCModel3 with a gamma-simulated 26-metabolite basis set containing MR-detectable metabolites present in gliomas. Metabolite CRLBs were compared using a paired two sample t-test, excluding values of 999 that indicate a lack of quantifiable metabolite in the spectrum. Differences in metabolite concentrations as a function of histologically-confirmed grade were determined with a one-way ANOVA. Post-hoc tests were performed using the Tukey-Kramer test. P values <.05 were considered significant.Results
Glioma tissue sample characteristics are presented in Table 1. Representative spectra acquired with FID and CPMG sequences are shown in Figure 1. Metabolite CRLBs for lactate and myo-inositol were significantly lower for the CPMG compared to the FID sequence (Table 2). While there were no differences observed for the other metabolites, most metabolites could be quantified with LCModel from spectra acquired with CPMG but many metabolites were not detectable in the FID spectra (Table 2). For example, lactate was quantifiable from 3 of the spectra acquired with FID compared to 12 spectra acquired with CPMG. A sample LCModel fitted spectrum acquired with the CPMG sequence is shown in Figure 2.
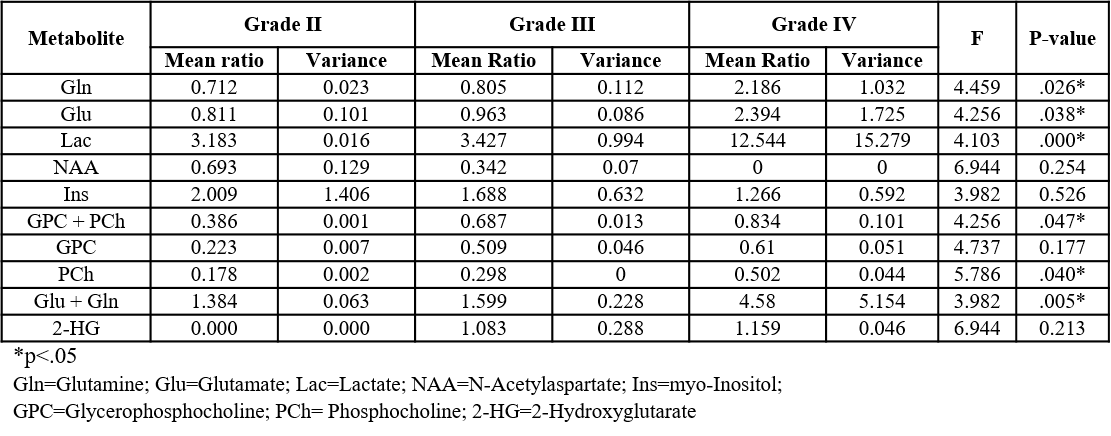
Comparison of metabolites concentrations as a function of WHO grade resulted in significant differences for most metabolites (Table 3). 2-hydroxyglutarate (2-HG) was also detected in approximately half of the isocitrate dehydrogenase (IDH)-mutated samples using both sequences.
Discussion
Metabolite CRLBs calculated from the CPMG sequence varied significantly from the FID sequence for two metabolites quantified, and most brain metabolites were quantifiable with LCModel from spectra acquired with the CPMG sequence. While FID sequences facilitate simultaneous quantification of metabolites, macromolecules, and lipid signals, the use of the CPMG sequence eliminates errors in quantification due to overlapping resonances and metabolites are more reliably quantified using LCModel. LCModel has the advantage of better separation of overlapping resonances compared to commonly reported manual peak integration methods, supporting the use of operator-independent methods for fitting high-resolution ex vivo NMR spectra. More accurate simulation of the macromolecule and lipid contributions to the baseline may enable improved LCModel analysis of FID spectra.
The concentration ratios relative to creatine plus phosphocreatine for lactate and glutamine plus glutamate were significantly higher in grade IV samples (post-hoc tests), consistent with prior literature.4 Metabolites such as glutamate and glutamine, which were expected to increase with grade,5 significantly varied as a function of grade but were not significant in post-hoc tests, suggesting the need for a larger sample size. Half of the samples with an IDH mutation had quantifiable 2-HG concentrations from 1D CPMG sequences. Typically, all IDH-mutated tissue should produce 2-HG. However, these results are promising as 2-HG can be difficult to quantify in 1D spectra due to overlap with many other metabolites.6
Conclusion
LCModel can reliably quantify HRMAS spectra acquired with the CPMG sequence but is less reliable from spectra acquired with the FID sequence. Increases in lactate and glutamine plus glutamate concentrations as a function of tumor grade were consistent with previous results using HRMAS for glioma metabolic analysis, and 2-HG was detected in 1D HRMAS spectra acquired with both sequences.Acknowledgements
This research was supported by an Emory University Department of Radiology & Imaging Sciences Seed Grant, and in part by the Cancer Tissue and Pathology Shared Resource of Winship Cancer Institute of Emory University (NIH/NCI P30CA138292). Solid-state HRMAS experiments were performed with the support of the Emory NMR Center.
References
- Suzuki H, Aoki K, Chiba K, et al. Mutational Landscape and Clonal Architecture in Grade II and III Gliomas. Nature Genet., 2015;47(5): 458-468.
- Wen P, Kesari, S. Malignant Gliomas in Adults. N Engl J Med., 2008;359(5):492-507.
- Provencher, S.W. Estimation of Metabolite Concentrations from Localized in Vivo Proton NMR Spectra, Magn Reson Med., 1993;30(6): 672-679.
- Kim JH, Chang KH, Na DG, et al. 3T 1H-MR Spectroscopy in Grading of Cerebral Gliomas: Comparison of Short and Intermediate Echo Time Sequences AJNR Am J Neuroradiol., 2006;27(7): 1412-1418.
- Takano T, Lin JHC, Arcuino G, et al. Glutamate release promotes growth of malignant gliomas. Nat Med. 2001;7(9):1010-1015.
- Wolfgang, B, Gilbert, H, Morteza, E, et. al. 1D-spectral editing and 2D multispectral in vivo 1H-MRS and 1H-MRSI: Methods and applications. Anal Biochem. 2017;529:48-64.
Figures