2277
Blood plasma metabolic profiling discriminates prostate cancer patients with metastases from those without metastases1Department of NMR and MRI Facility, All India Institute of Medical Sciences, New Delhi, India, 2Department of Urology, All India Institute of Medical Sciences, New Delhi, India, 3Department of Radio-diagnosis, All India Institute of Medical Sciences, New Delhi, India, 4Department of Pathology, All India Institute of Medical Sciences, New Delhi, India
Synopsis
The present study evaluates the metabolic profile of blood plasma for distinguishing prostate cancer (PCa) patients with metastases (n=30) and without metastases (n=35) using 1H-NMR spectroscopy. Our data showed significant lower concentration of leucine, valine, isoleucine, glycerophosphocholine, glutamine and acetoacetate in PCa patents with metastases as compared to patients without metastases. Results provided an insight into the alterations in the metabolic pathways in PCa and indicated that NMR spectroscopy may help in determining potential biomarker/s for the diagnosis of PCa patients with metastases.
Purpose: To investigate the blood plasma metabolic profiling to distinguish PCa patients with metastases from those without metastases using 1H-NMR.
Introduction: Prostate cancer (PCa) with metastasis is fatal disease requiring early diagnosis and effective treatment. Aggressive PCa metastasize or spread to bones, such as the hip, spine and pelvis bones. Current diagnostic methods cannot predict metastatic PCa at a treatable stage of the disease. Metastatic PCa is considered advanced stage. Thus, the aim of this study is to distinguish the metabolite profile of blood plasma of PCa patients with metastases and those without metastases and for determining novel potential biomarker/s of aggressive PCa.
Methods: Blood samples were collected from metastases PCa patients [(n = 30 mean age: 67.1± 8.6 years), PSA; 542.15 (47.72- 4166.60) ng/mL] and from those without established metastases [(n =35, mean age: 66.8 ± 8.0 years), PSA; 59.0 (5.56- 331.70) ng/mL, in morning pre-prandial after overnight fasting. An informed consent was taken and the study was approved by Institute Ethics Committee. Each blood sample was centrifuged at 3000 rpm for 10 minutes at 4°C and plasma was separated and stored at -80°C until NMR experiments were carried out. Proton spectra of blood plasma samples were carried out at 700 MHz spectrometer (Agilent, USA) using 1D CPMG with presaturation. The following parameters were used for 1D NMR: 64 scan, with a 70s relaxation delay and a spectral width of 9124.1 Hz with an echo time of 15ms. Two dimensional (2D) TOCSY experiment was carried out for assignments of metabolite peaks. For comparison between these two patient groups, unpaired Mann-Whitney U test was carried out using SPSS software (SPSS Inc. Chicago, IL, USA). A p-value <0.05 was considered significant. Univariate (receiver operating characteristics (ROC) curve analysis) and multivariate (orthogonal partial least squares–discriminant analyses (OPLS-DA), variable importance to projection (VIP) score statistical analysis was carried out using MetaboAnalyst 4.0.
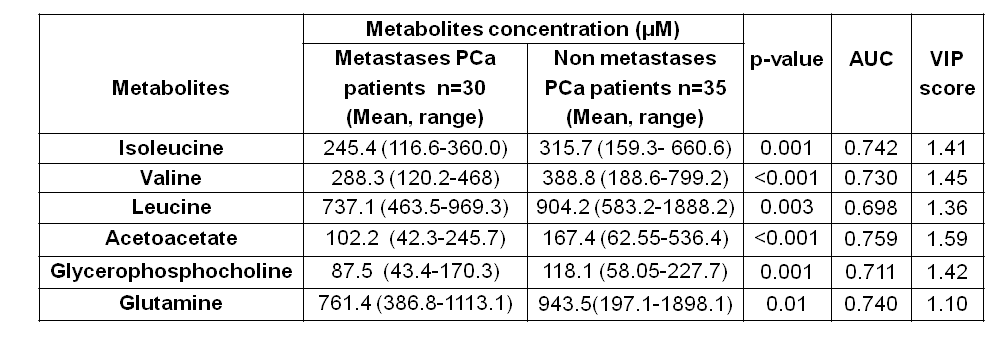
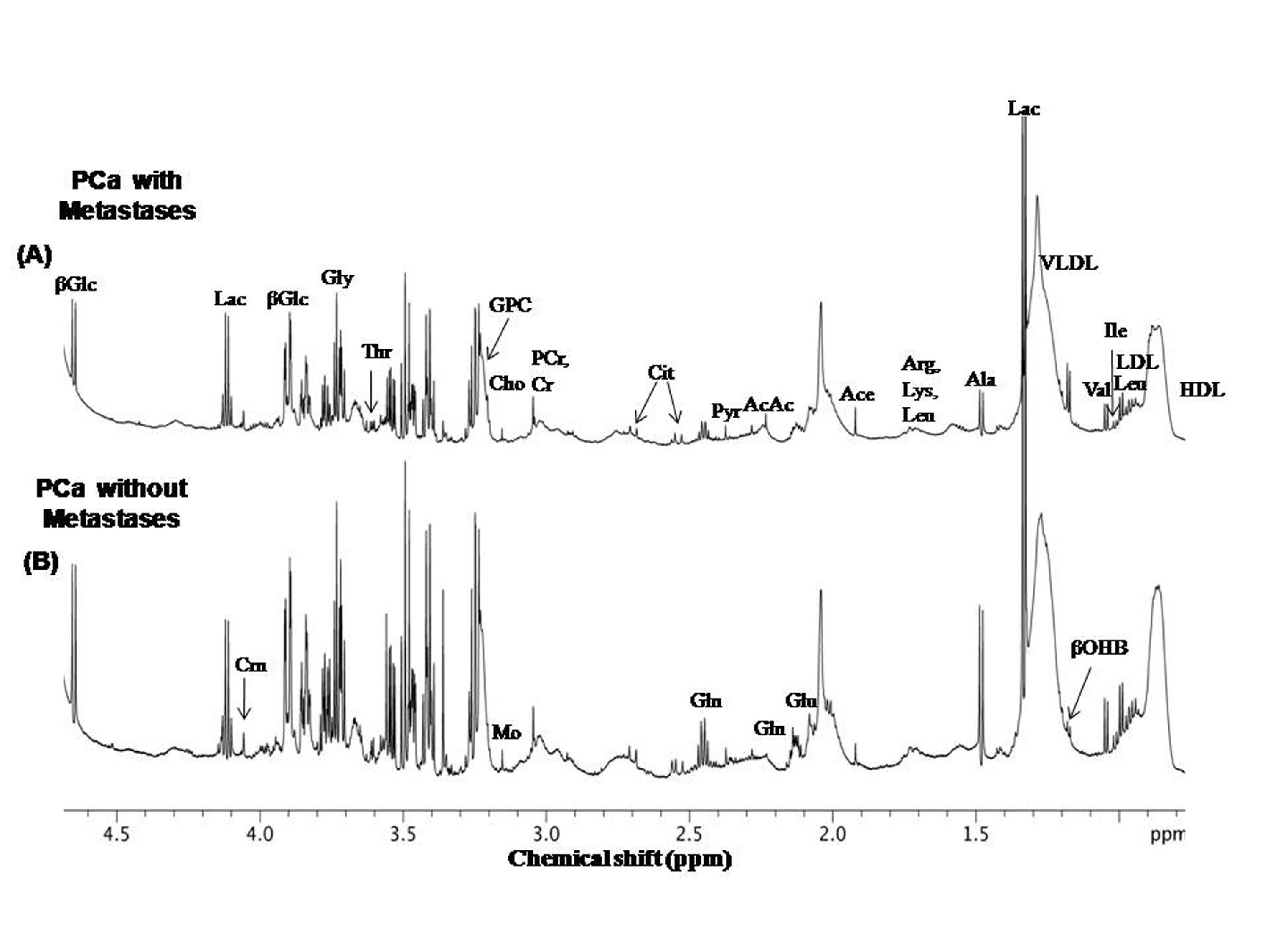
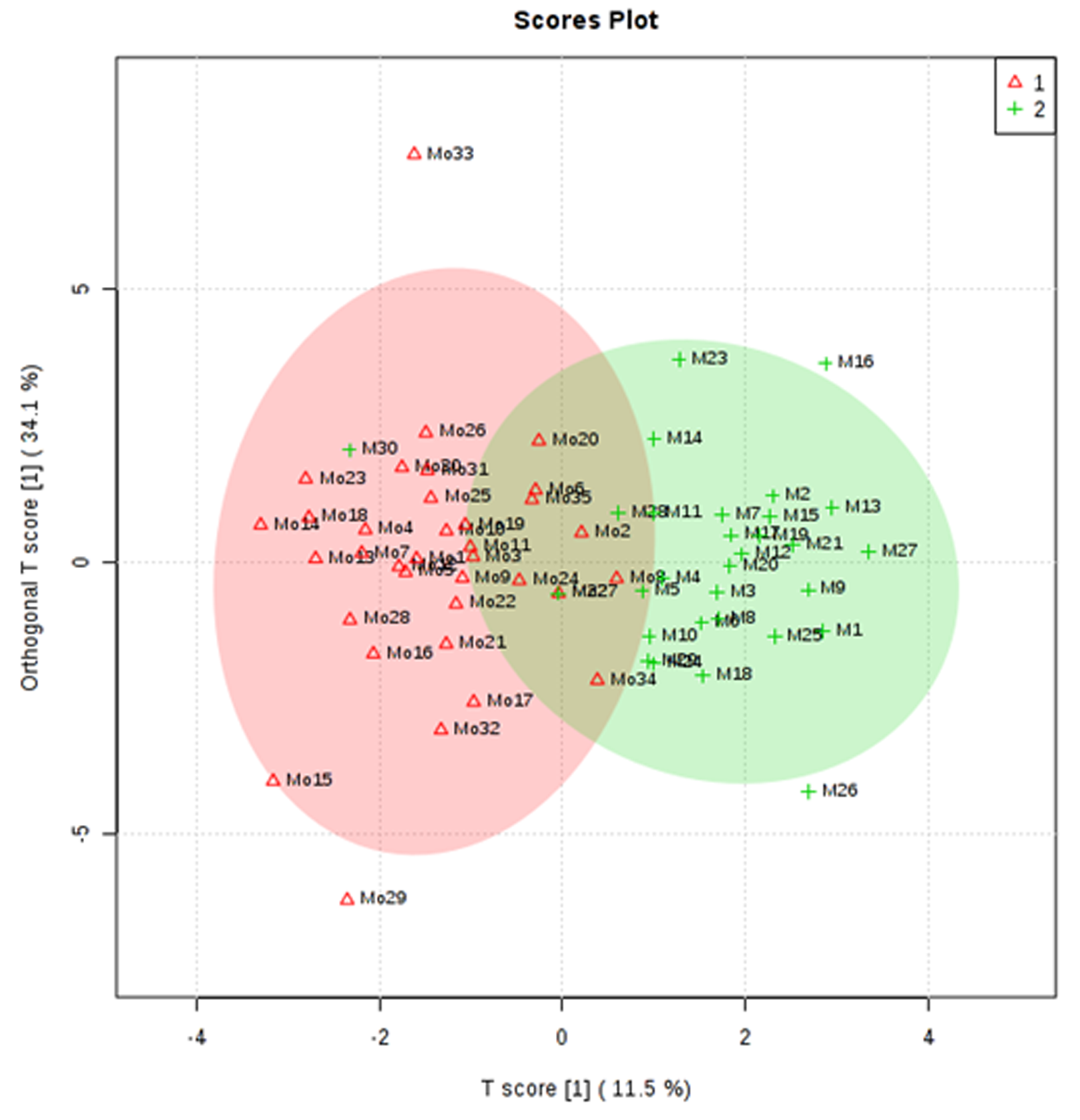
Results: Figure 1 shows the representative aliphatic region of 1D 1H NMR spectrum of blood plasma sample of a PCa patient with metastases (A) and from a patient without metastases (B). In all, 29 metabolites were assigned using 1D and 2D NMR. For the concentration [μM (mean, range)] of 6 metabolites that showed significant (p<0.05) differences, the AUC values and VIP scores (>1) between the two groups were determined and presented in Table 1. Figure 2 shows the OPLS -DA score plot showing the discrimination of PCa patients with metastases from those without metastases.
Discussion: Our data revealed a significantly lower concentration of branch chain amino acids (BCAAs) such as valine (Val), leucine (Leu) and isoleucine (IIe) in the blood plasma of metastases PCa patients compared to those without metastases. This indicated the utilization of BCAAs for increased protein turnover in aggressive PCa1. Our data also showed significantly lower concentration of glutamine (Gln) in patients with metastases. In metastatic PCa cells, glutaminolysis is predominantly performed by enzyme glutaminase. Gln also has an important role in the maintenance of lipogenesis as well as to provide intermediate for the Kreb’s cycle through glutaminolysis2. Furthermore, our data showed significantly decreased concentration of membrane metabolite glycerophosphocholine (GPC) in the blood plasma of patients with metastases indicating a higher proliferation of metastatic PCa cells3. A lower level of ketone body acetoacetate (AcAc) was seen in metastases PCa patients. These are produced by liver from fatty acids oxidation and then converted into acetyl CoA, which then enters the TCA cycle. Lower level of AcAc may be reflecting increased utilization of lipid demands to meet the energy requirements for cell growth and proliferation in metastatic cncer cells4. Univariate ROC curve analysis indicated that AcAc showed high AUC of 0.759 while Leu had an AUC of 0.698. The VIP scores of Val, IIe, Leu, GPC, Gln and AcAc were increased in aggressive PCa, which indicated that these metabolites play an important role in distinguishing PCa patients with metastases compared to those without metastases. Figure 2 is a representative multivariate analysis OPLD-DA score plot, showing clear discrimination between metastases PCa patients compared to those without metastases.
Conclusion: This study demonstrated that NMR based metabolomics may be useful for distinguishing PCa patients with and without metastases. Further our results provided a better understanding of the metabolic pathway alterations through changes in amino acids, phospholipids, fatty acids oxidation and glutaminolysis are associated with PCa progression and tumorgenesis.
Acknowledgements
NRJ acknowledges SERB, Government of India for the J.C. Bose Fellowship, while PK for UGC fellowship.References
(1). Dereziński P, Klupczynska A, Sawicki W et al. Int J Med Sci. 2017; 14(1): 1–12. (2). Wang Q, Hardie RA, Hoy AJ et al. J Pathol. 2015; 236:278–289. (3). Giskeødegård GF, Hansen AF Bertilsson H et al. Bri J Cancer. 2015; 113(12):1712–1719. (4). Puchalska P & Crawford PA. Cell Metab.2017; 25(2):262–284.Figures