2223
Free-breathing Whole-heart Magnetic Resonance Angiography with Self-gated Radial Phyllotaxis Trajectory1Cardiology, Boston Children's Hospital, Boston, MA, United States, 2Pediatrics, Harvard Medical School, Boston, MA, United States, 3Informatics, Technical University of Munich, Garching, Germany
Synopsis
Whole-heart magnetic resonance angiography is commonly performed with diaphragmatic navigator gating to compensate for respiratory motion, but this approach is inefficient as data must be reacquired when it is outside the acceptance window. We therefore developed and validated a self-gated respiratory motion compensation technique based on a radial phyllotaxis k-space trajectory in which all data are accepted throughout the respiratory cycle.
Introduction
Whole-heart magnetic resonance angiography (MRA) is an important clinical tool to diagnose coronary abnormalities without the use of ionizing radiation.1 Nevertheless, a robust, time-efficient method to compensate for the respiratory motion of the heart remains elusive.2 Requiring patients to hold their breath imposes a limit on scan time that is currently too brief to produce images with sufficient spatial-resolution. Consequently, most recent whole-heart MRA steady-state free precession (SSFP) techniques employ various methods to compensate for respiratory motion during free-breathing acquisitions. Commonly, this is performed by using a diaphragmatic navigator to track right hemi-diaphragm displacement in order to limit data collection to a portion of the respiratory cycle. This approach is inherently inefficient as image data outside the acceptance window must be reacquired, thus prolonging the scan time by ≈2-fold. To address this deficiency, we implemented a radial phyllotaxis trajectory for respiratory self-gated free-breathing whole-heart MRA acquisition.3,4Method
We developed a modified radial phyllotaxis trajectory for 3D whole-heart MRA SSFP acquisitions. The modified radial phyllotaxis trajectory has N projections that are sorted into M interleaves with P projections (i.e., N=MxP). The number of projections in each interleaf (i.e., P) is determined by the number of acquired k-space data in each shot (i.e., TFE factor). The number of interleaves, therefore, is the number of beats (i.e., shots) required to acquire the whole k-space data. The first projection in each interleaf was oriented along the superior-inferior (SI) direction for respiratory self-gating. To minimize the amount of gradient changes within each interleaf, the number of interleaves is rounded to the closest Fibonacci number (Fig. 1).
We implemented the modified radial phyllotaxis trajectory for the electrocardiogram (ECG) triggered 3D whole-heart MRA SSFP sequence on a 1.5T scanner (Philips, Achieva dStream). To minimize cardiac motion artifacts, the k-space data are divided into multiple shots (interleaves), each of which is acquired at the quiescent period of the cardiac cycle over 80-120 ms (Fig. 2). T2-preparation and fat-saturation pre-pulses precede the k-space data acquisition to enhance the contrast between the blood and myocardium and to minimize the signal from fat. After the image acquisition, the signal from the first projection (k-space line) in each interleaf was transformed into image domain and used for respiratory motion detection. The first projection in the first interleaf was correlated on the first projection in the other interleaves to measure the respiratory motion in each shot. The estimated respiratory motion was then used to correct for the k-space data.
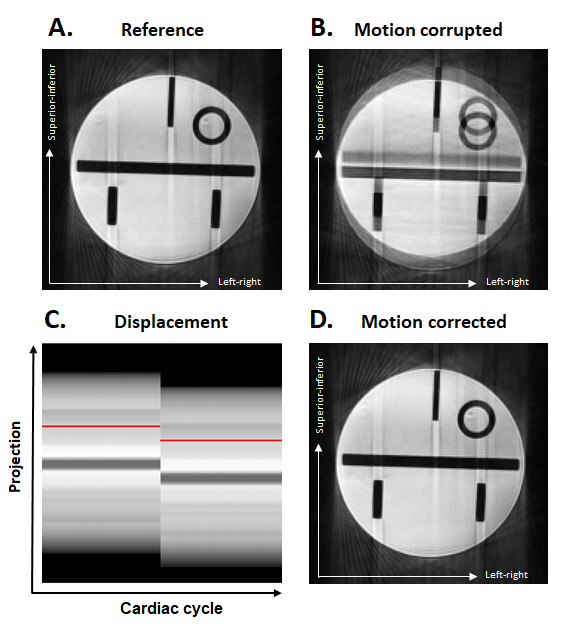
To assess the efficacy of this technique, a phantom and an in-vivo study were performed. A phantom was imaged with the ECG triggered 3D whole-heart MRA SSFP sequence with the following parameters: FOV 250 mm, resolution 1.5 mm, flip angle 60°, TR/TE 3.2/1.57 ms, 610 interleaves, and TFE factor 30. The scan was paused in the middle of acquisition, to move the phantom and produce motion in the SI direction. At the end of the scan, the k-space data were extracted and the self-gating signal from the first projection in each interleaf was used for correcting the motion in the k-space data. The corrected and uncorrected k-space data were reconstructed using a 3D NUFFT technique5 to generate motion corrected and motion corrupted images.
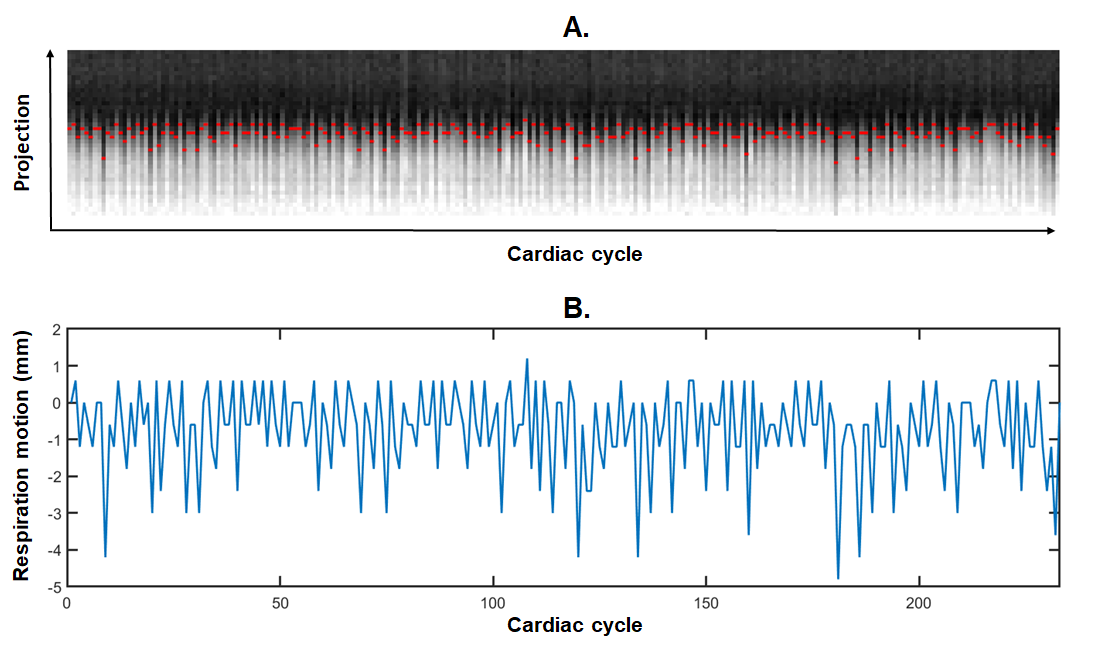
A 27-year-old male patient with congenital heart disease was imaged using the same sequence after the injection of 0.2 mmol/kg Gadovist contrast agent with the following imaging parameters: FOV 200 mm, resolution 1.52 mm, flip angle 60°, TR/TE 3.1/1.56 ms, 233 interleaves, and TFE factor 30. After the image acquisition, the k-space data were corrected for the respiratory motion using the first projection in each interleaf. The corrected k-space data were then reconstructed off-line using a 3D NUFFT technique.
Results
Fig. 3 shows the phantom images acquired with 3D whole-heart MRA SSFP sequence without motion (A) and with motion (B). The pattern of induced motion and motion corrected images are shown in Fig 3 (C, D). The scan time for the phantom study was ~10 minutes. Fig. 4 shows the pattern of respiratory motion in the patient during the free-breathing 3D whole-heart MRA SSFP acquisition. The acquisition time was ~4 minutes. The motion corrected images of the patient in axial, sagittal, and coronal views are shown in Fig. 5.Conclusion
We developed a radial phyllotaxis trajectory for respiratory self-gated free-breathing acquisition of 3D whole-heart MRA SSFP sequence. Future work will include examining this technique on more patients and extending it for 3D cine and late gadolinium enhancement imaging.Acknowledgements
No acknowledgement found.References
1. Chiribiri A, Botnar RM, Nagel E. Magnetic resonance coronary angiography: where are we today? Curr Cardiol Rep. 2013 Feb;15(2):328.
2. Scott AD, Keegan J, Firmin DN. Motion in cardiovascular MR imaging. Radiology. 2009 Feb;250(2):331-51.
3. Stehning C, Börnert P, Nehrke K, Eggers H, Stuber M. Free-breathing whole-heart coronary MRA with 3D radial SSFP and self-navigated image reconstruction. Magn Reson Med. 2005 Aug;54(2):476-80.
4. Piccini D, Feng L, Bonanno G, Coppo S, Yerly J, Lim RP, Schwitter J, Sodickson DK, Otazo R, Stuber M. Four-dimensional respiratory motion-resolved whole heart coronary MR angiography. Magn Reson Med. 2017 Apr;77(4):1473-1484.
5. Knoll, F.; Schwarzl, A,; Diwoky, C.; Sodickson DK.: gpuNUFFT - An Open-Source GPU Library for 3D Gridding with Direct Matlab Interface. Proc ISMRM p4297 (2014).
Figures