2217
A swine model of selective coronary stenosis using transcatheter delivery of a 3D printed implant for MR imaging: Feasibility and EfficacyCaroline M. Colbert1,2, Jiaxin Shao2, Jesse W. Currier3, Olujimi A. Ajijola4, Rohan Dharmakumar5, Sandra M. Duarte-Vogel2,6, Peng Hu1,2, and Kim-Lien Nguyen1,2,3
1Physics and Biology in Medicine Graduate Program, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 2Department of Radiological Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 3Division of Cardiology, David Geffen School of Medicine at UCLA and VA Greater Los Angeles Healthcare System, Los Angeles, CA, United States, 4UCLA Cardiac Arrhythmia Center and Division of Cardiology, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 5Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, and Division of Cardiology, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 6Department of Laboratory Animal Medicine, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States
Synopsis
This study aims to investigate the feasibility and efficacy of a closed-chest method for coronary stenosis creation in swine models of ischemic heart disease (IHD). We successfully deployed high-resolution 3D printed intracoronary implants in three healthy swine subjects using a transcatheter angioplasty delivery approach. All subjects underwent angiography and MR cine imaging for assessment of ventricular regional wall motion. At post-mortem dissection, we successfully retrieved the implants. These results support early feasibility and efficacy of our proposed approach for applications including stress testing, infarct creation, and evaluation of diagnostic techniques or therapeutics in swine models of IHD.
Introduction
Animal models with focal coronary artery stenosis are important tools for imaging studies of ischemic heart disease (IHD), because the severity of the coronary stenosis relates to the burden of myocardial ischemia. Coronary stenosis can be induced in animal models using atherogenic diets, but this method does not give reliable control over the location or degree of stenosis formation.1 Precise control of coronary stenosis can be achieved with ameroid constrictors,2 but placement of these devices requires open-chest surgery. One minimally-invasive method has been described but requires implantation of tapered nylon coronary occluders for MR and SPECT imaging.3 These occluders are challenging to manufacture and have not been studied in a wide range of sizes. Using MR imaging, we aim to demonstrate the feasibility and efficacy of a closed-chest method for coronary stenosis creation by combining high-resolution 3D printed intracoronary implants with a transcatheter angioplasty delivery approach in swine models of IHD.Methods
We designed intracoronary implants with a range of sizes using Autodesk® Tinkercad® (Autodesk Inc., San Rafael, California). The implants were smooth, hollow 3D printed tubes with rounded edges (Fig. 1). Several practical constraints limited the dimensions of the implants. The outer diameter was limited to fit inside a typical coronary guide catheter. The inner diameter could be no less than the size of a deflated coronary angioplasty balloon. The minimum wall thickness of the tubes was 0.3 mm and their length ranged from 2.6 to 4.0 mm for maneuverability. The implants were printed from Formlabs Grey Resin (Formlabs Inc., Somerville, MA) using a Formlabs Form 2 3D printer with a minimum XY feature size of 150 µm. The implants were dip-coated with a 25% heparin solution (Surface Solutions Laboratories, Inc., Carlisle, MA) to prevent thrombus formation. After general anesthesia, femoral arterial access, and adequate anticoagulation with intravenous heparin (5000 – 10000 units) was achieved in three swine subjects, the implants were deployed under fluoroscopic guidance. One implant was placed in either the LAD (subjects 1 and 2) or the LCX (subject 3). The implant was delivered to the most distal segment of the artery that it securely fit. After deployment, angiograms in two orthogonal views were acquired for visual estimation of stenosis severity. Subjects were immediately transferred to the MR suite to undergo MRI. To evaluate regional wall motion abnormalities (RWMA), post-ferumoxytol enhanced cine images were obtained using gradient echo sequences. Two subjects underwent adenosine stress testing. Subjects were humanely euthanized. Hearts were excised and dissected to locate and retrieve the intracoronary implants.Results
Implants were successfully delivered in all three subjects. A clear focal coronary stenosis was achieved using fluoroscopic guidance, and implants did not migrate. All subjects underwent successful MR cine imaging without device-related image artifacts. Subjects 1 and 2 had no RWMA at rest, while subject 3 had lateral wall hypokinesis (Fig. 2). Subjects 1 and 2 underwent MRI adenosine stress tests without complications. Subject 3 developed ventricular fibrillation shortly after cine imaging and died. At post-mortem dissection for case 2 and 3, coronary implants were successfully retrieved from the same segment of the artery in which they were placed. In case 2, the implant showed no intraluminal thrombus formation (Fig. 3).Discussion
These results support early feasibility and efficacy of 3D printed epicardial coronary implants for MR imaging studies in swine models of IHD. Applications range from stress testing to infarct creation to evaluation of diagnostic techniques or therapeutics. Successful implant delivery with MR documentation of regional wall motion and angiographic visualization of focal coronary stenosis support the feasibility of this method for future MR studies. The absence of RWMA in subjects 1 and 2 and the presence of abnormalities in subject 3 indicate that these implants have potential to induce a range of ischemic burden. The successful retrieval of two implants from their placement positions suggests that they do not migrate following delivery. Subject survival in cases 1 and 2, and lack of thrombus formation in case 2, demonstrate potential use of this method in future survival studies.Conclusion
Our MR imaging and angiographic results support preliminary feasibility and efficacy of a combined 3D printed epicardial coronary implant and transcatheter delivery approach in swine models. If confirmed in larger studies, the proposed technique has potential to impact the broader practice of MR imaging research with large animal models of IHD.Acknowledgements
This work was supported by American Heart Association Transformational Award 18TPA34170049, NHLBI R01HL127153, and pilot funding from the UCLA Department of Medicine and the UCLA Department of Radiological Sciences. We thank the UCLA Lux Lab for providing 3D printing services. We also thank Dr. Dara Kraitchman for discussions about her work with nylon occluders.References
- Kramsch D, Aspen A, Abramowitz B, et al. Reduction of coronary atherosclerosis by moderate conditioning exercise in monkeys on an atherogenic diet. N Engl J Med. 1981;305(25):1483-1489.
- Litvak J, Siderides L, Vineberg A. The experimental production of coronary artery insufficiency and occlusion. Am Heart J. 1957;53(4):505-518.
- Kraitchman D, Bluemke D, Chin B, et al. A minimally invasive method for creating coronary stenosis in a swine model for MRI and SPECT imaging. Invest Radiol. 2000;35(7):445-451.
Figures
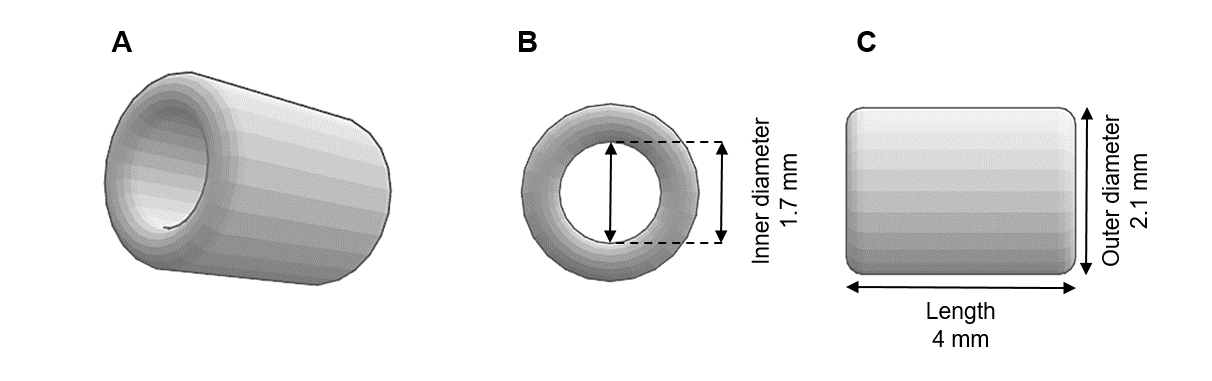
Images show (A)
oblique view, (B) front view and (C) side view of an implant design with 2.1 mm
outer diameter, 1.7 mm inner diameter and 4.0 mm length.
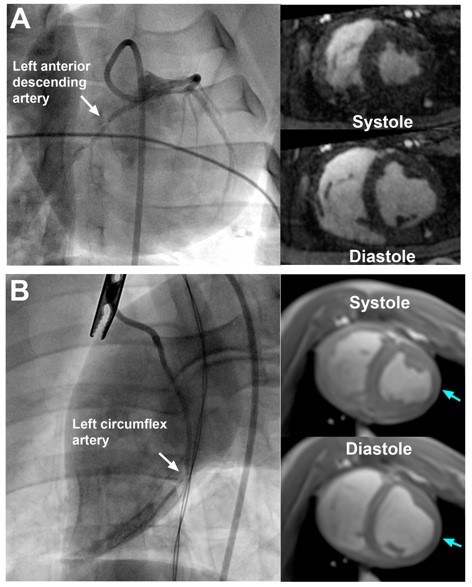
Fluoroscopic
images show deployment of the 3D printed coronary implant in the (A) left
anterior descending artery (LAD, white arrow) and (B) left circumflex artery
(LCX, white arrow) along with corresponding cine MR images. The blue arrows
point to hypokinesis of the lateral wall.
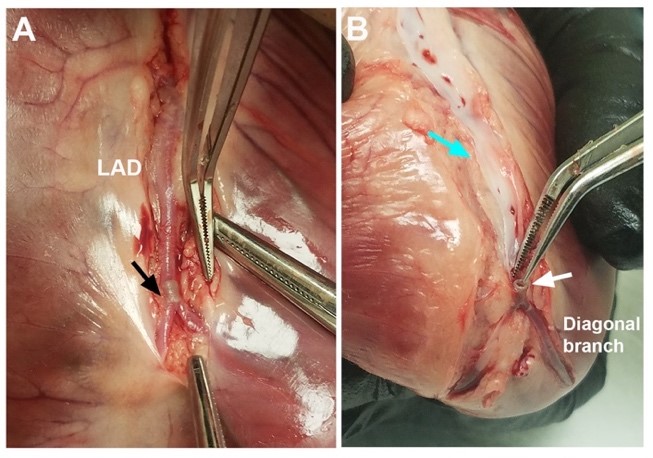
Post-mortem
images confirm (A) location and successful retrieval of 3D printed coronary
implants (black arrow), (B) absence of coronary endothelial damage (blue
arrow), and absence of thrombus formation (white arrow). LAD, left anterior
descending artery.