2212
Retrospective analysis of pulmonary transit time in different patient samples and recording conditions.1Cardiology, CHWAPI, Tournai, Belgium, 2Radiology, CHWAPI, Tournai, Belgium, 3Institut de Myologie, Hôpital Pitié-Salpétrière, aphp, Paris, France, Metropolitan, 4Institut de Myologie, CEA, DRF, IBFJ, MIRCen, NMR Laboratory, Paris, France, Metropolitan
Synopsis
A retrospective analysis of pulmonary transit time and intra-pulmonary blood volume in Becker dystrophic myopaths at 3T and unselected patients / cardiopaths and normals at 1,5 T.
Background or Purpose
The follow-up of patients suffering from cardiologic diseases leading to heart failure lacks of robust markers of bad clinical outcome. Ejection fraction, although clearly linked to survival, is not a very good discriminant between those who will show a poor clinical condition, multiple hospitalizations and those who will keep in relatively good physical shape for the following years. Pulmonary transit time has shown some promises as a marker of bad clinical condition. We aimed to study this particular parameter estimated from first-pass perfusion images and specifically assessed how it correlates with the standard volumetric measurements of the heart.Methods
We retrospectively studied 2 groups of patients: Group 1/ patients with Becker muscular dystrophy (n=37) from the Becker Heart Study, imaged at the Institute of Myology (Pitié-Salpêtrière, Paris, France) at 3T (Siemens Trio/PrismaFit) and injected manually; Group 2/ Consecutive patients (ischemic, hypertrophic, myocarditis, inflammatory… excluding significant valvular regurgitation but including aortic stenosis. n= 126), examined in CHWAPI (Tournai, Belgium) at 1,5 T (Siemens Aera and AdvantoFit) and injected with an automatic contrast media injector. Cine images were acquired using a balanced steady-state-free precession (bSSFP) sequence in a stack of short-axis oriented slices encompassing the left ventricle. Usual indices of right and left ventricular function were analyzed. Peak ejection rate (PER) was estimated as the minimum value of the dV/dt curve. Perfusion imaging was acquired using a saturation recovery Turbo-FLASH sequence in short axis oriented slices repeated 80 or 100 times to capture the first pass. For both groups, ROIs were analyzed in right ventricular and left ventricular cavities through the first pass of contrast media (Dotarem Guerbet 0.1 ml/kg) in the basal short axis view. The pulmonary transit time (PTT) was calculated according to Mischi et al. [1], fitting a log-normal function to the actual patient data. Intra-pulmonary blood volume (IPBV) was computed as IPBV = PTTxCO [1] where CO is the cardiac output as given by the Simpson’s rule volume calculations.Results
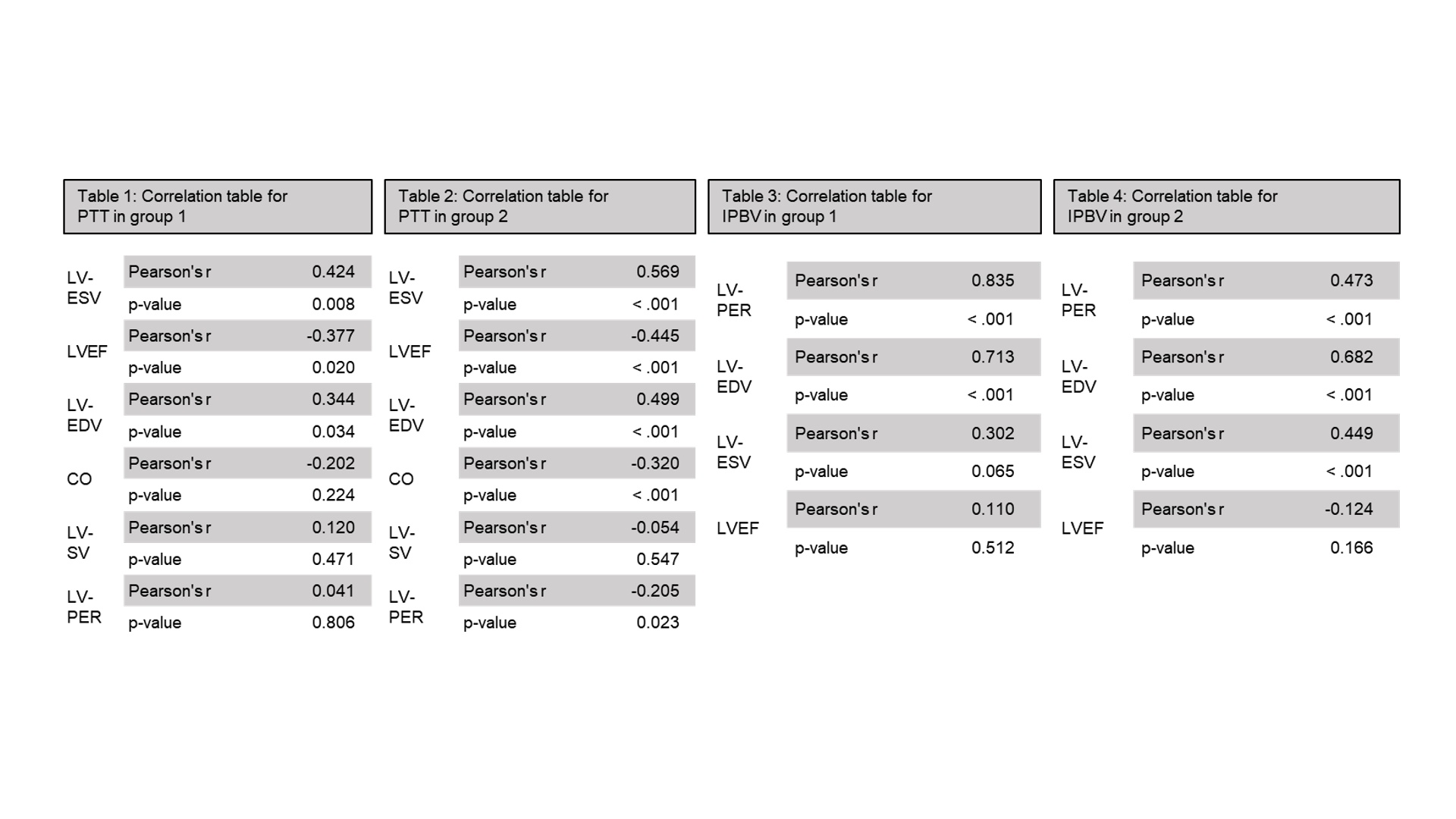
In Group 1, the patients came from a homogeneous population and showed no sign of significant cardiac failure although demonstrating a wide range of LVEF. We observed statistically significant correlations between PTT and the volumetric measurements (table 1). In group 2, although the population presented a diversity of diseases and conditions (some were just hospitalized for heart failure: HFPEF or HFREF), the correlations were very similar (table 2). We also correlated IPBV with some variables for both groups excluding LV-SV and CO as they are part of its computing in the first place (table 3 and 4). It should be noted that EDV, ESV and LVEF were correlated as well as SV and PER (data not shown).Conclusions
In this study, we demonstrated correlations between PTT, IPBV, and different volumetric parameters. We confirmed and expanded the results of Herold et al. [2] to various patient types and recording conditions. These correlations were consistent throughout different patient populations, MR acquisition techniques and magnetic fields. The diversity of conditions that were studied and gave similar results, enhances our confidence in the robustness of the findings. The lack of dependence between PTT and SV or PER could allow for a specific discrimination of the normal, the failing heart and the high output state. These preliminary results clearly await further studies to establish their clinical relevance.Acknowledgements
No acknowledgement found.References
[1] Mischi, M., H.C.M. van den Bosch, J.a. den Boer, J. Verwoerd, R.J.E. Grouls, C.H. Peels, et H.H.M. Korsten. « Intra-thoracic blood volume measurement by contrast magnetic resonance imaging ». Magnetic Resonance in Medicine 61, no 2 (2009): 344–353.
[2] Herold, Ingeborg H F, Salvatore Saporito, Massimo Mischi, Hans C van Assen, R Arthur Bouwman, Anouk G W de Lepper, Harrie C M van den Bosch, Hendrikus H M Korsten, et Patrick Houthuizen. « Pulmonary transit time measurement by contrast-enhanced ultrasound in left ventricular dyssynchrony ». Echo Research and Practice 3, no 2 (2016): 35–43.
Figures