2208
Simultaneous T1 and T2 Mapping with MOLLI Acquisition: Proof of Concept1University of California San Francisco, San Francisco, CA, United States, 2GE Heathcare, Palo Alto, CA, United States
Synopsis
MOLLI is known to underestimate T1 values. Instead of fitting MOLLI data to an ideal but unrealistic exponential inversion recovery model, we simulated signal evolution incorporating actual scan parameters based on which we improved T1 mapping as well as demonstrated the feasibility of deriving T2 mapping simultaneously.
INTRODUCTION
Quantitative tissue parametric mapping, such as T1 and T2 mapping, has become as a promising tool for tissue characterization. MOdified Look-Locker Inversion Recovery (MOLLI) [] has being widely used for cardiac T1 mapping, which acquires data at multiple inversion times (TIs) from different heartbeats during inversion recovery (IR) in a single breath-hold scan. However, due to known complications, including incomplete inversion recovery within limited breath-hold time, disruption of imaging data acquisition to signal recovery and inevitable cardiac variations, MOLLI tends to underestimate T1 values and be biased by the T2 of the tissue. Instead of fitting MOLLI data to an ideal but unrealistic exponential inversion recovery model conventionally used, in this work, we explored a new method to simulate signal evolution incorporating actual scan parameters based on which we derive T1 mapping with improved accuracy and potentially T2 values simultaneously.MATERIALS AND METHODS
As a proof of concept, this study investigated the feasibility of simultaneous T1/T2 mapping using MOLLI data, (3-(3)-3-(3)-5) [1], collected from five cardiac patients scanned on a 1.5T MR scanner (GE Medical Systems, Milwaukee, WI). SMART1Map based on saturation recovery (SR), which provides more accurate T1 measurements [2], were also collected as the reference in this study.
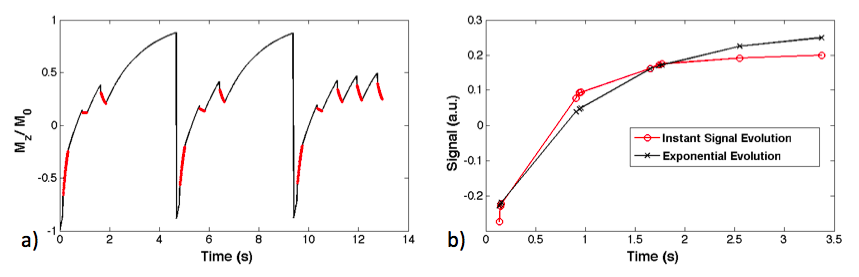
The specific parameters of patient scans were used for numerical simulation of the instant signal evolutions. Figure 1a shows the simulated signal evolution (Mz/M0) of static tissues underging the entire inversions/recoveries/data sampling process, based on T1/T2=1000/50ms (myocardium), three inversion pulses, TR/TE=3/1.3ms, FA=65o, heart rate=76 bpm, trigger delay= 450 ms, and 64 bSSFP readouts with 5 dummy pulses. In Figure 1b the signals at different TIs simulated with instant evolution are plotted (red line with circles), and those generated with the exponential recovery (A-B*exp(-TI/T1)) is also plotted (black line with crosses).
A dictionary of signal evolution curves was built, given T1:[500:1500], T2;[20:150] for myocardium at 1.5 T. Signals in the acquired data were fit to the dictionary of simulated signal evolutions to derive T1 and T2 that present lowest fitting error. This study is to show the proof of concept of using MOLLI data for simultaneously deriving T1 and T2 maps (so called MOLLI-T1T2 method).
RESULTS AND DISCUSSION
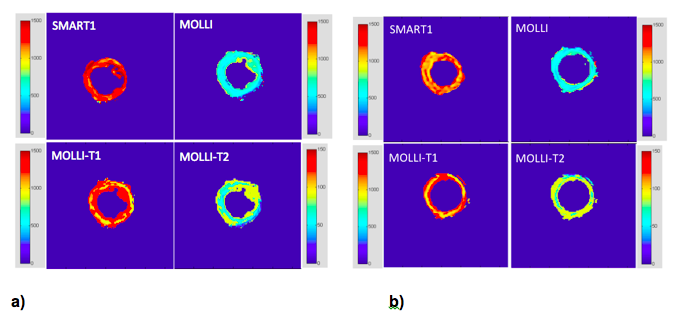
Figure 2 shows two representative cases, with T1 maps from the conventional MOLLI, SMART1, and MOLLI-T1T2 methods, as well as T2 map derived with MOLLI-T1T2.
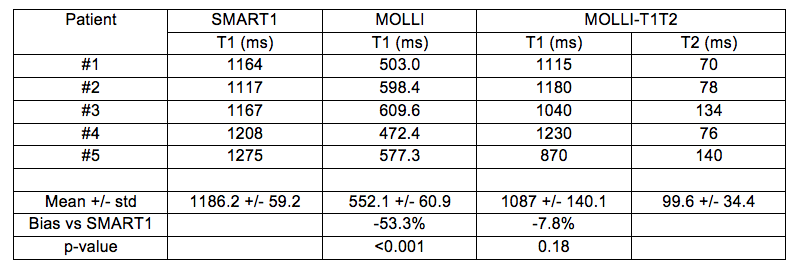
Table 1 summarizes the measurements averaged within a ROI in the septum wall. With reference to the T1 values obtained with SMART1, the conventional MOLLI largely underestimated the T1 values of the myocardium, which is larger than many of the previously reported numbers, could be contributed to the use of relatively large flip angle of 65 degrees. In comparison, the proposed method provides much more accurate T1 estimation, while the T2 estimation needs further validation.
Magnetization transfer needs to be further included to improve the simulation model. Cardiac cycle duration was assumed fixed in our initial test, which should be more specific at each heartbeat during the scan.
CONCLUSIONS
Our preliminary results show the feasibility of deriving both T1 and T2 maps from MOLLI acquisition. The derived T1 values are shown to be greatly improved compared to the conventional exponential data fitting used by MOLLI. Further investigations are needed to improve the accuracy of T2 mapping, such as including magnetization transfer and taking into account of cardiac variations during the scan to improve the simulation model.Acknowledgements
NIH R56HL133663 (JL), GE Healthcare Research Grant (JL)References
1. Messroghil D. et al, Modified Look‐Locker inversion recovery (MOLLI) for high‐resolution T1 mapping of the heart. MRM, v52, p141, 2004.
2. Slavin G. et al, True T1 mapping with SMART1Map (Saturation method using adaptive recovery times for cardiac T1 mapping): a comparison with MOLLI. JCMR, V15, 2013.
Figures