2204
Structural Changes in Cardiac Allograft Vasculopathy Patients after One Year Post Heart Transplantation1Northwestern Radiology, Northwestern, Chicago, IL, United States, 2Northwestern, Chicago, IL, United States
Synopsis
Cardiac MRI demonstrates differences between heart transplant recipients more than one year post-HTx and controls using T2, T1 and ECV. Our study demonstrated elevated global T2 and ECV, and segmental T1 in HTx patients when compared to controls. This may provide further insight into the complex pathophysiology of this disease process, which includes a chronic and subacute component. CMR could potentially be implemented as an adjunct to the current methods of detecting CAV (intravascular ultrasound and invasive coronary cineangiography)
Introduction
After the first year post heart transplantation(HTx), patients are at risk for cardiac allograft vasculopathy(CAV) leading to significant mortality1 CAV is monitored with invasive coronary angiography (ICA) as the gold standard which is limited by insensitivity to detect early disease2.The pathophysiology of CAV has not been completely elucidated3. It is proposed that immunological and vascular factors result in diffuse fibromuscular intimal hyperplasia, in addition to atherosclerotic and vasculitic lesions4. Therefore, CAV is a combination of a chronic process with a subacute inflammatory component. As a non-invasive diagnostic alterative, cardiac MRI (CMR) has emerged as a promising tool for the assessment of global and regional changes in left ventricular (LV) structure and function. Our hypothesis is that CMR provides a structural assessment of CAV-related changes. These changes include LV fibrosis (pre-and post-contrast T1-mapping to quantify extracellular volume fraction (ECV))5, in addition to LV edema and active inflammation (assessed by T2-mapping)6, which could be suggestive of more advanced and progressive CAV.Methods
51 HTx patients greater than one year post-HTx (50±17 years, 31 males, time after HT=8±5 years) and 18 age-matched controls (49±15 years, 12 males) underwent CMR for structural analysis of the heart including T2-mapping6 as well as pre-and post-contrast T1-mapping using a MOLLI sequence7 at 3 short-axis locations (base, mid, apex). For structural parameters, data analysis was performed with commercial software (cvi42, Circle), and global values for LV native T1, T2 and ECV were calculated. ECV was calculated using pre‐and post-contrast T1‐maps and the patient's hematocrit level obtained the day of CMR. ECV was not calculated in 11 patients due to an inability to receive gadolinium contrast secondary to renal dysfunction or technical difficulties in the scan protocol. Measures of ventricular function were calculated from a stack of standard cine SSFP images of the heart using cvi42 (Circle). Patient CAV status was graded 0 to 3 based on the ISHLT CAV grading scale. Table 1 describes the angiographic criteria for each CAV grade2.Results
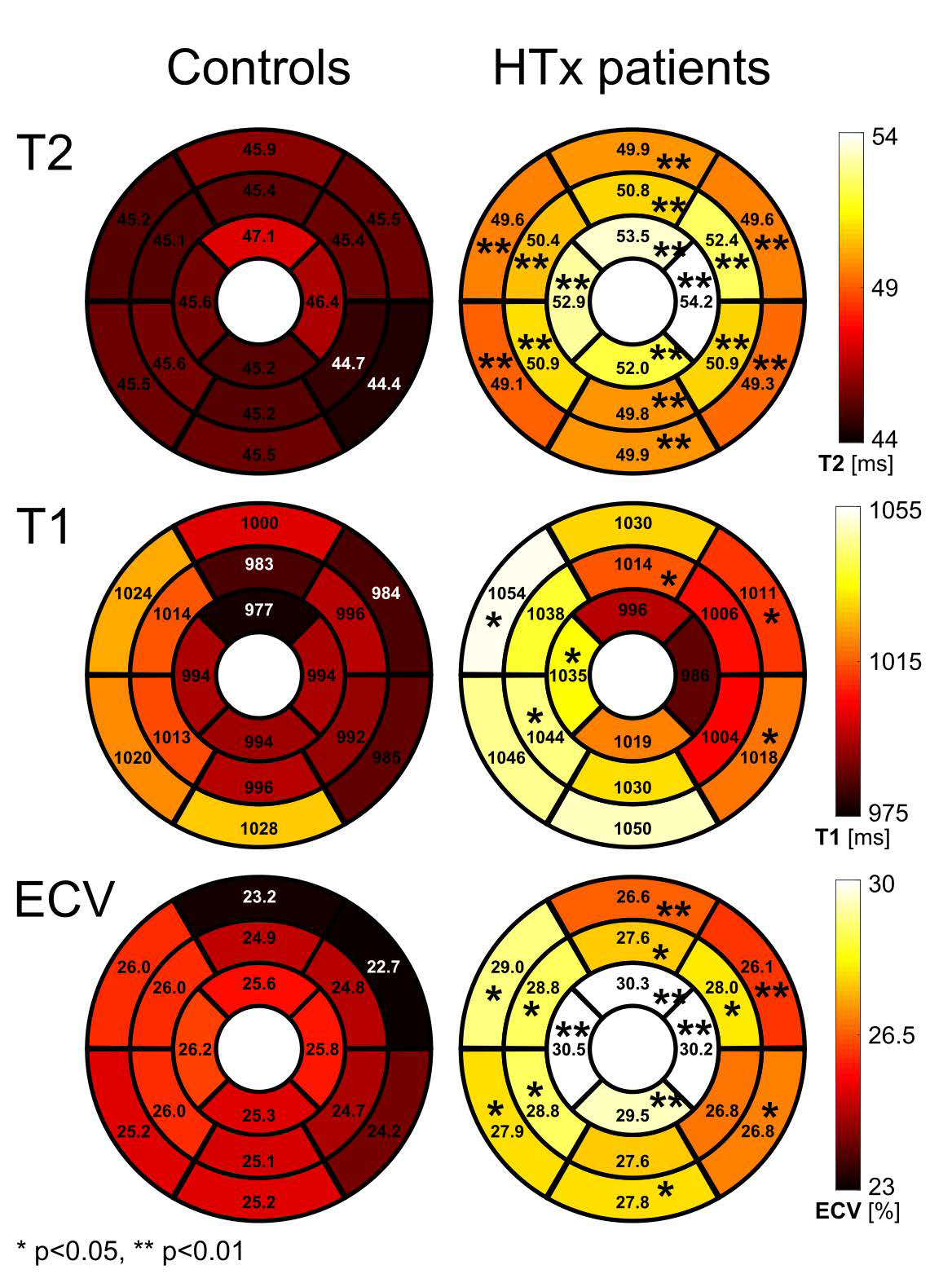
Study cohorts demographics are reported in Table 2. Figure 1 depicts a comparison of structural parameters (T1, T2 and ECV) between all CAV subgroups and controls. Figure 2 illustrates structural differences between all HTx patients and controls on a segmental level based on the 16-segment AHA model. All CAV subgroups demonstrated significantly elevated T2 when compared to controls (p<0.001). Specifically, CAV 0 demonstrated significantly elevated global T2 in comparison to controls (p<0.001). The CAV 2/3 group demonstrated significantly higher global T2 than CAV 1 group (p<0.01). On a segmental level, HTx patients demonstrated significantly higher T2 across all 16-segments (p<0.01). Global T1 was not statistically different among controls and CAV subgroups (p=0.09) globally. However, T1 was significantly elevated in 6/16 LV segments (p<0.05). Globally, ECV was elevated between HTx patients and controls (p<0.05). Furthermore, global ECV was elevated compared to controls for CAV1 (p<0.01) and CAV2/3 (p<0.05). On a segmental level, ECV was significantly higher in HTx patients in 14/16 segments, notably including all apical segments (p<0.05 in 8/14 segments, p<0.01 in 6/14 segments)Discussion
Previous studies have demonstrated that HTx patients have elevated T1, T2 and ECV when compared to controls8,9. Although CAV is considered a chronic condition, patients with more advanced and progressive CAV, causing accelerated luminal obstruction, have higher levels of inflammatory markers C-reactive protein and serum amyloid A10,11. Our study demonstrated elevated global T2 and ECV, and segmental T1 in HTx patients when compared to controls. Increased T2 in advanced CAV 2/3 in comparison to CAV 1 groups suggests a more active inflammatory process in these patients resulting in edema. Patients with insignificant CAV 0 using the gold standard ICA had elevated T2 when compared to controls, which may suggest inflammation and edema which is undetectable by ICA. Recent work has suggested that the complex pathophysiology may include a component of vasculitis which may extend into the surrounding myocardium and therefore could account for the increased T24. Significant T1 differences seen segmentally but not globally may be due to subclinical microvascular disease causing areas of focal inflammation, ischemia and fibrosis in a non-uniform fashion, which varies in its occurrence from patient to patient12,13.Conclusion
CMR provides structural information on both segmental and global levels. These parameters may be a useful adjunct to gold standard ICA to help detect early stage CAV, or detect more aggressive and advanced disease. Further studies with larger more uniform cohorts are warranted to further characterize the diagnostic value of T2, T1 and ECV in CAV detection.Acknowledgements
No acknowledgement found.References
1. Lund LH, Khush KK, Cherikh WS, Goldfarb S, Kucheryavaya AY, Levvey BJ, Meiser B, Rossano JW, Chambers DC, Yusen RD, Stehlik J, International Society for H, Lung T (2017) The Registry of the International Society for Heart and Lung Transplantation: Thirty-fourth Adult Heart Transplantation Report-2017; Focus Theme: Allograft ischemic time. J Heart Lung Transplant 36 (10):1037-1046. doi:10.1016/j.healun.2017.07.019
2. Mehra MR, Crespo-Leiro MG, Dipchand A, Ensminger SM, Hiemann NE, Kobashigawa JA, Madsen J, Parameshwar J, Starling RC, Uber PA (2010) International Society for Heart and Lung Transplantation working formulation of a standardized nomenclature for cardiac allograft vasculopathy-2010. J Heart Lung Transplant 29 (7):717-727. doi:10.1016/j.healun.2010.05.017
3. Lu WH, Palatnik K, Fishbein GA, Lai C, Levi DS, Perens G, Alejos J, Kobashigawa J, Fishbein MC (2011) Diverse morphologic manifestations of cardiac allograft vasculopathy: a pathologic study of 64 allograft hearts. J Heart Lung Transplant 30 (9):1044-1050. doi:10.1016/j.healun.2011.04.008
4. Lee MS, Tadwalkar RV, Fearon WF, Kirtane AJ, Patel AJ, Patel CB, Ali Z, Rao SV (2018) Cardiac allograft vasculopathy: A review. Catheter Cardiovasc Interv. doi:10.1002/ccd.27893
5. Moon JC, Messroghli DR, Kellman P, Piechnik SK, Robson MD, Ugander M, Gatehouse PD, Arai AE, Friedrich MG, Neubauer S, Schulz-Menger J, Schelbert EB, Society for Cardiovascular Magnetic Resonance I, Cardiovascular Magnetic Resonance Working Group of the European Society of C (2013) Myocardial T1 mapping and extracellular volume quantification: a Society for Cardiovascular Magnetic Resonance (SCMR) and CMR Working Group of the European Society of Cardiology consensus statement. J Cardiovasc Magn Reson 15:92. doi:10.1186/1532-429X-15-92
6. Giri S, Chung YC, Merchant A, Mihai G, Rajagopalan S, Raman SV, Simonetti OP (2009) T2 quantification for improved detection of myocardial edema. J Cardiovasc Magn Reson 11:56. doi:10.1186/1532-429X-11-56
7. Messroghli DR, Radjenovic A, Kozerke S, Higgins DM, Sivananthan MU, Ridgway JP (2004) Modified Look-Locker inversion recovery (MOLLI) for high-resolution T1 mapping of the heart. Magn Reson Med 52 (1):141-146. doi:10.1002/mrm.20110
8. Miller CA, Sarma J, Naish JH, Yonan N, Williams SG, Shaw SM, Clark D, Pearce K, Stout M, Potluri R, Borg A, Coutts G, Chowdhary S, McCann GP, Parker GJ, Ray SG, Schmitt M (2014) Multiparametric cardiovascular magnetic resonance assessment of cardiac allograft vasculopathy. J Am Coll Cardiol 63 (8):799-808. doi:10.1016/j.jacc.2013.07.119
9. Dolan RS, Rahsepar AA, Blaisdell J, Lin K, Suwa K, Ghafourian K, Wilcox JE, Khan SS, Vorovich EE, Rich JD, Anderson AS, Yancy CW, Collins JD, Markl M, Carr JC (2018) Cardiac Structure-Function MRI in Patients After Heart Transplantation. J Magn Reson Imaging. doi:10.1002/jmri.26275
10. Pethig K, Heublein B, Kutschka I, Haverich A (2000) Systemic inflammatory response in cardiac allograft vasculopathy: high-sensitive C-reactive protein is associated with progressive luminal obstruction. Circulation 102 (19 Suppl 3):III233-236
11. Fyfe AI, Rothenberg LS, DeBeer FC, Cantor RM, Rotter JI, Lusis AJ (1997) Association between serum amyloid A proteins and coronary artery disease: evidence from two distinct arteriosclerotic processes. Circulation 96 (9):2914-2919
12. Abu-Qaoud MS, Stoletniy LN, Chen D, Kerstetter J, Kuhn M, Pai RG (2012) Lack of relationship between microvascular and macrovascular disease in heart transplant recipients. Transplantation 94 (9):965-970. doi:10.1097/TP.0b013e31826accca
13. Fearon WF, Hirohata A, Nakamura M, Luikart H, Lee DP, Vagelos RH, Hunt SA, Valantine HA, Fitzgerald PJ, Yock PG, Yeung AC (2006) Discordant changes in epicardial and microvascular coronary physiology after cardiac transplantation: Physiologic Investigation for Transplant Arteriopathy II (PITA II) study. J Heart Lung Transplant 25 (7):765-771. doi:10.1016/j.healun.2006.03.003
Figures