2190
Effect of nicotine administration on myocardial perfusion under adenosine stress: A dynamic investigation using cine-ASL in mice.1Aix-Marseille Univ, CNRS, CRMBM, Marseille, France
Synopsis
We have monitored
myocardial perfusion (MBF) dynamically under pharmacologically-induced stress
in mice using a time-optimized cine-ASL MRI approach with about 2.5min temporal
resolution. One main advantage of the repeatable cine-ASL in this context is to
monitor MBF during successive stress episodes in the same animal allowing for
internal control. In this study we clearly demonstrated that single bolus nicotine
administration (1mg·kg-1) significantly reduced perfusion by 35%
under adenosine stress (tail vein continuous infusion, 90µg·kg-1·min-1) in healthy mice.
INTRODUCTION
Although it is generally accepted that replacement nicotine therapies and smokeless tobacco consumption (that can include electronic cigarettes) are less detrimental compared to smoking in the general population, the negative health effects of nicotine alone remain controversial1-3. We aimed at investigating the acute effect of nicotine on myocardial blood flow (MBF) under stress conditions in vivo using arterial spin labeling (ASL). The cine-ASL method4 was optimized for temporal resolution to enable dynamic quantification of myocardial perfusion throughout an adenosine stress protocol in mice.METHODS
MBF was quantified dynamically in 7 mice (C57BL6; 24.4±6.4g; 4 Females) at rest and under adenosine stress with or without nicotine on a 7T Pharmascan (Bruker) using a 1H 4-channel Bruker CryoProbe receive array. Mice were anesthetized with 1.5% isoflurane mixed in 100% O2 (1L·min-1). MBF maps were acquired using cine-ASL4 in short-axis view. Acquisition time was reduced using two-fold GRAPPA acceleration and segmented acquisition resulting in a temporal resolution of approximately 2.5min depending on heart (HR) and breathing rate (BR). Three stress tests were performed consecutively under (i) control condition, and (ii) with nicotine or (iii) saline solution injected in addition. Myocardial stress was obtained by adenosine infusion (90µg·kg-1·min-1) via an intravenous tail catheter. Nicotine (1mg·kg-1) or saline solution was added via intraperitoneal bolus injection 1) concomitantly with adenosine stress induction and 2) at maximal vasodilation. The effect of the injection alone was evaluated during a third stress episode replacing nicotine with saline solution. Complete MBF recovery was ensured between two consecutive stresses (Figure1). The effect of nicotine injection on resting perfusion was evaluated separately on 3 mice. Left ventricular (LV) function under each condition was approximated by measuring the diastolic and systolic LV areas on long-axis views. MBF was quantified at end-diastole in the anterior LV using home-made IDL software4. For each condition, baseline and maximal perfusion values were determined as the average of the 3 measurements preceding the onset and end of adenosine infusion, respectively. Repeated-measures ANOVA was performed to detect differences between conditions.RESULTS
MBF at baseline and maximal vasodilation were not significantly different across conditions. Perfusion reserve calculated in control (2.63±0.57) and saline (2.30±0.58) conditions were not significantly different (Table1). Following nicotine injection under maximal vasodilatation, the reserve decreased to 1.46±0.47, whereas baseline MBF changes due to nicotine administered at rest were not significant. MBF response to adenosine stress was significantly reduced in presence of nicotine: 1) When concomitantly injected with stress induction, nicotine prevented rapid MBF onset. In presence of nicotine, the time to reach 85% of maximum MBF under adenosine stress was doubled compared to control condition and following saline injection (Table 1). 2) Under maximal vasodilatation state, nicotine injection resulted in a 34.8±6.8% MBF decrease lasting for 11.7±1.3min. During nicotine injection, an initial short transient (<40s) BR increase (+35.5±6.9rpm) and HR drop (-100±43bpm compared to the pre-injection value). As opposed to BR, HR recovered to a lower value compared to control condition but was not different under saline condition (Table1). Such changes were not observed during control saline injection. The estimated LV volumes were not significantly different across conditions.DISCUSSION
One clear advantage of the repeatable cine-ASL technique for this study was the ability to monitor MBF during 3 stress episodes in a single animal providing a “control stress” situation for internal comparison. On average, adenosine infusion took 5min to provoke maximum vasodilation and to return to baseline MBF after arrest of infusion. These times are much shorter than those previously observed in rats (~10min)5 and likely due to the higher blood turnover in mice compared with rats. The reduction of MBF after nicotine injection under stress disappeared gradually within 12min, which is in line with the rapid blood elimination of this drug in mice (half-life~6min)6. This finding is corroborated by the prolonged time to reach maximum stress when adenosine infusion was started simultaneously with the nicotine injection (12 vs 5min). These findings, in agreement with previous reports of coronary impaired endothelial-dependent vasodilation in humans3 and large animals7,8, demonstrate that nicotine diminished the vasodilatory response to pharmacological stress in healthy myocardium, potentially exposing the myocardium to increased ischemic risk in situations of increased metabolic demand, such as exercise or pathological conditions. In that regard, nicotine has been shown to worsen myocardial dysfunction in regionally “stunned,” ischemic myocardium in dogs9.CONCLUSION
We used a sequential MRI perfusion mapping protocol and demonstrated in vivo that nicotine diminished perfusion reserve under adenosine infusion by 37%. Further studies should investigate continuous infusion of nicotine to investigate whether a dose-dependence exists and to establish more detailed functional consequences on overall cardiac function and associated risk factors.Acknowledgements
We acknowledge funding from: Agence Nationale de la Recherche grant ANR-14-CE17-0016 COFLORES; Fondation de la Recherche Médicale grant FRM DBS20140930772 and France Life Imaging grant ANR-11-INBS-0006.References
1 Benotwitz NL, Gourlay
SG. Cardiovascular toxicity of nicotine: implications for
nicotine replacement therapy. J Am Coll
Cardiol. 1997; 29: 1422.
2 Benotwitz NL, Burbank
AD. Cardiovascular toxicity of nicotine: Implications for
electronic cigarette use Trends Cardiovasc Med. 2016 Aug;26(6):515-23.
3 Kaijer L, Berglund B. Effect of nicotine on coronary blood-flow in man. Clin Physiol. 1985; 5;541.
4 Troalen T, Capron T,
Cozzone PJ, Bernard M, Kober F. Cine‐ASL: A steady‐pulsed arterial spin
labeling method for myocardial perfusion mapping in mice. Part I. Experimental
study. Magn Reson Med. 2013 Nov;70(5):1389.
5 Troalen T, Kenmoe C, Cozzone P,
Bernard M, Kober F. Dynamic of the perfusion reserve during adenosine-induced
stress in rats. In: Magnetic Resonance Materials in Physics, Biology and
Medicine. Vol. 26 Suppl 1. ESMRMB:
30th Annual Scientific Meeting Toulouse/FR, Oct 3-5; 2013. p. 68.
6 Petersen DR, Norris
KJ, Thompson JA. A comparative study of the disposition of nicotine and its
metabolites in three inbred strains of mice. Drug Metab Dispos. 1984
Nov-Dec;12(6):725-31.
7 Mehta MC, Jain AC,
Billie MD. Combined effects of cocaine and nicotine on cardiovascular
performance in a canine model. Clin.
Cardiol. 2001;24,620-626.
8 Young MA, Knight DR,
Vatner SF. Parasympathetic coronary vasoconstriction induced by nicotine in
conscious calves. Circ Res. 1988; 62:891.
9 Przyklenk K. Nicotine exacerbates postischemic contractile dysfunction of stunned
myocardium in the canine model: possible role of free radicals. Circulation 1994. 89:1272–1281
Figures

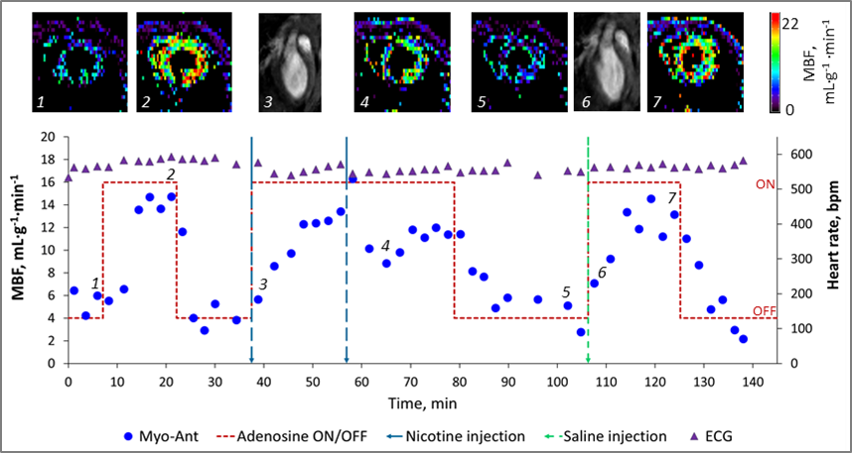

Table 1: MBF is myocardial blood flow; max refers to the maximum reached under stress condition and baseline to MBF in absence of adenosine. * † indicates significant difference with control and saline condition, respectively