2187
Initial Experience with MR-Based Respiratory and Cardiac Motion-Corrected PET/MR Imaging of the Coronary Arteries1Icahn School of Medicine at Mount Sinai, New York, NY, United States, 2Weill Cornell Medicine, New York, NY, United States, 3University Hospital of Brest, Brest, France, 4British Heart Foundation Centre for Cardiovascular Science, Edinburgh, United Kingdom, 5Mount Sinai St Luke's Hospital, New York, NY, United States
Synopsis
A major advantage of hybrid PET/MR systems is the radiation-free high spatial and temporal resolution of MR imaging that can be used to estimate cardio-respiratory motion present during PET data acquisition. This information can be incorporated into reconstruction algorithms to correct for motion in the PET data to reduce blurring and increase target-to-background ratios (TBR) of PET hotspots. This may be of particular importance in cardiac imaging where the heart is in constant motion. In this work, we report our initial experience applying cardio-respiratory motion-corrected PET/MR to 18F-sodium fluoride PET/MR imaging of the coronary arteries.
Purpose
Recently, the PET tracer 18F-sodium fluoride has been shown to identify culprit coronary artery plaque in patients following myocardial infarction using PET/CT 1, and has been explored using PET/MR 2. Despite these successes, the substantial respiratory and cardiac motion during PET data acquisition limits the image quality and potentially degrades the qualitative and quantitative assessment of tracer uptake and potentially affects the detection of disease. Using temporally-resolved 3D cardiac MRI, hybrid PET/MR has the potential to provide motion correction for coronary PET imaging at no additional radiation dose, potentially significantly improving evaluation of PET data. Recently, the feasibility of motion-corrected cardiac PET/MR has been demonstrated for measuring 18F-FDG uptake in the myocardium for detection of inflammation in a group of patients with cardiac sarcoidosis3. In this work, we report our initial experience with these tools for identifying 18F-sodium fluoride uptake in the coronary artery of patients with coronary artery disease (CAD).Methods
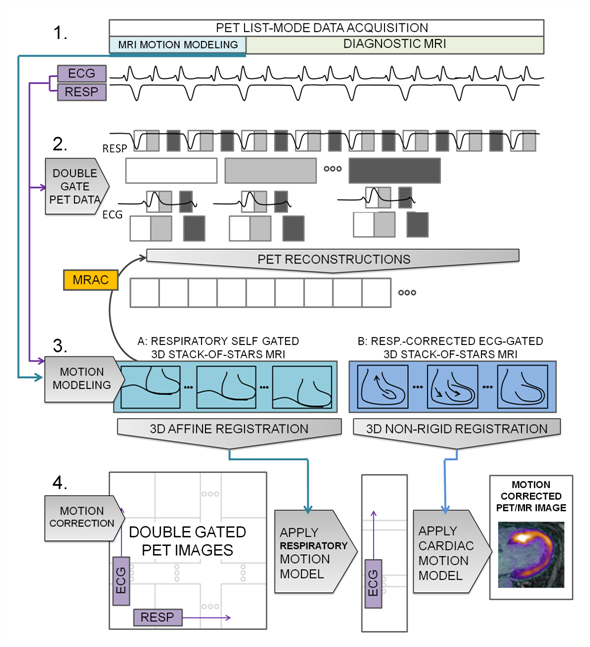
Three patients with coronary artery disease underwent hybrid PET/MR (Biograph mMR, Siemens) which included a previously described method of MR-based motion modeling and a PET reconstruction using a retrospective reconstruct-transform-average (RTA) motion correction approach3. 18F-sodium fluoride (10 mCi) was administered 60 minutes prior to imaging. List-mode PET data acquisition lasted for 50 minutes. Respiratory motion was estimated using a free-breathing 3D golden-angle radial stack-of-stars sequence (based on Siemens bodyCompass 4). A whole-body coronal slab with 3x3x3mm-resolution and 1600 spokes was acquired over 6-7min. The amplitude of the center of k-space was used to provide an estimate of the respiratory phase during the acquisition. Spokes were then divided into 4 respiratory frames based on signal amplitude and reconstructed in Matlab using NUFFT algorithms5. Motion vector fields (MVFs) between respiratory frames were then estimated using freely-available non-rigid registration algorithms6. Cardiac motion was estimated separately using a similar acquisition but with higher resolution of 1.4x1.4x1.4mm and a coronal slab just covering the heart. In addition, contrast-enhancement (infusion of 0.2mmol/kg Multihance, Bracco) provided additional image-contrast between the blood-pool, coronary vessels and myocardium. Respiratory phase was estimated in the same manner before finding the actual head-to-foot displacement from the images. k-Space data were phase-shifted to correct for the head-to-foot displacement. Corrected k-space data were then sorted into 3 cardiac frames based on recorded ECG trigger timing before offline reconstruction. MVFs between cardiac frames were then estimated. Motion correction of PET data employed the reconstruct-transform-average (RTA) approach. Double-gated list-mode PET data were reconstructed offline (e7tools, Siemens) using an iterative algorithm (OP-OSEM, 3 iterations, 21 subsets). Attenuation correction maps2 of the body were transformed using the estimated respiratory MVFs. Finally, RTA was performed in two steps. All cardiac frames were transformed to the end expiration position using corresponding MVFs. Then each respiratory-motion-corrected cardiac frame was transformed to the diastolic position using the cardiac MVFs before averaging all frames (Fig. 1). Non-motion corrected non-gated (non-MC non-gated), double respiratory and cardiac gated (gated) and double respiratory and cardiac motion corrected (MC) 18F-sodium fluoride-PET images were evaluated qualitatively for image blurring and overall quality. An experienced reader identified regions of elevated uptake coinciding with the coronary arteries on fused PET and MRA images and rated the difference in appearance before and after motion correction.Results
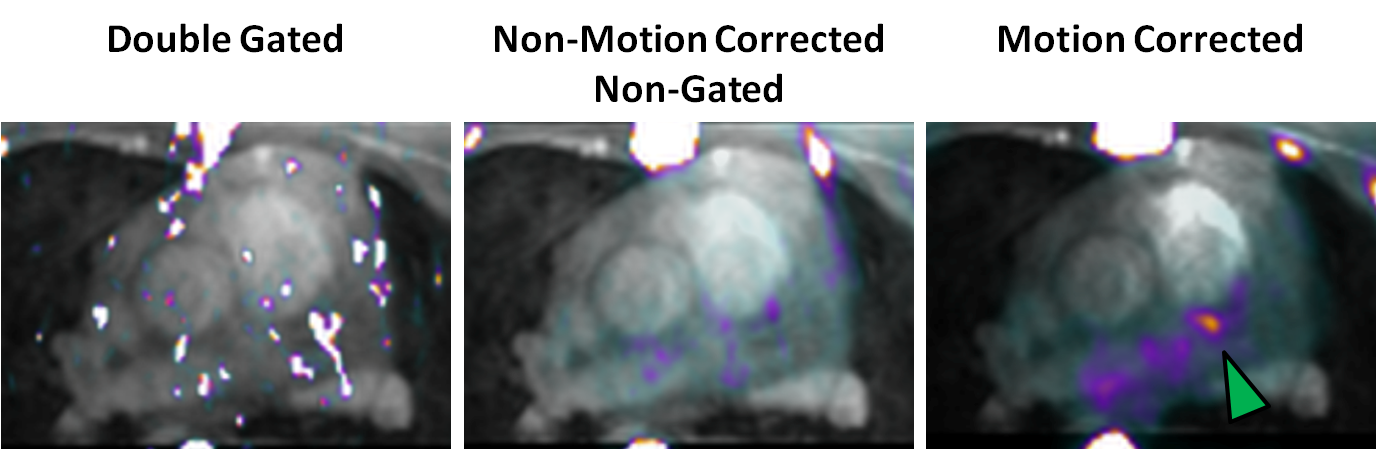
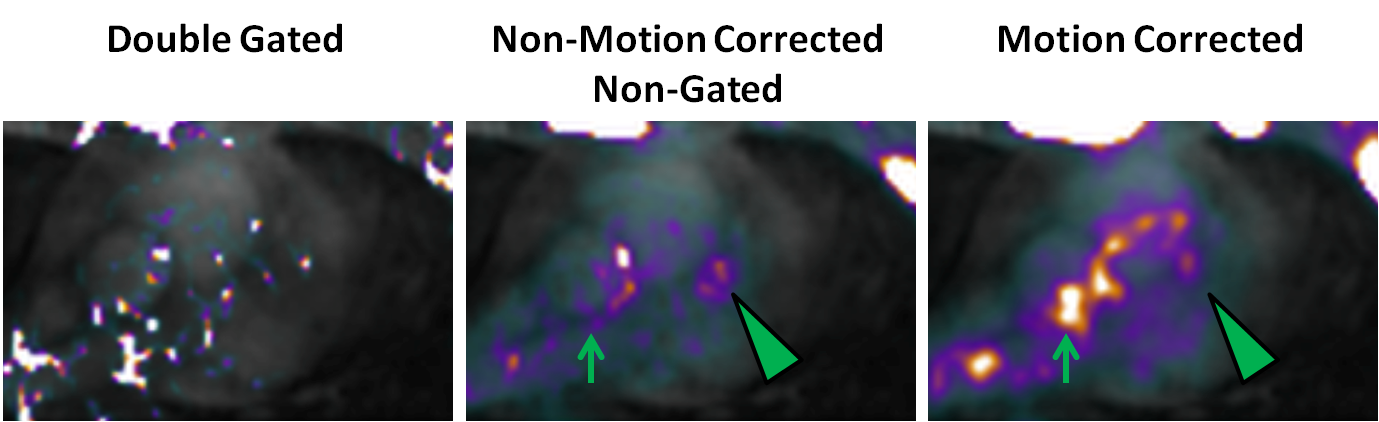
All three patients exhibited regions of increased 18F-sodium fluoride uptake in the coronary arteries (arrowheads in figures). The focal nature of the uptake and alignment with proximal segments of the left coronary artery, a common area of plaque formation, gave reasonable confidence in these hotspots’ designation as active disease. In patient 1 a region of increased 18F-sodium fluoride uptake was observed on the left anterior descending (LAD) coronary artery only after motion correction of the PET data (Fig. 2). In patient 2 a diffuse region of uptake on the coronary artery appeared more focal after motion correction (Fig. 3). In patient 2 the impact of motion correction on surrounding background signal can be seen (arrow). In this small cohort, motion correction tended to amplify background signal in the blood pool. In all cases, double gated PET images were too noisy to identify focal uptake on the coronary arteries.Discussion
Our initial experience applying motion correction tools, previously validated in cardiac PET/MR, to the coronary arteries has shown the potential of motion corrected coronary PET/MR by identifying a lesion that was not observed on non-motion corrected non-gated PET images. A more rigorous assessment of the methodology and potential optimizations for the small coronary arteries are now required to assess clinical impact.Acknowledgements
This work was supported by NIH grant R01 HL071021. The authors gratefully acknowledge clinical research coordinators Stella Palencia, Miguel Bravo and Renata Pyzik.References
1. Joshi NV, Vesey AT, Williams MC et al, Lancet. 2014 Feb 22;383(9918):705-13
2. Robson PM, Dweck MR, Trivieri MG et al. Coronary Artery PET/MR Imaging: Feasibility, Limitations, and Solutions. JACC Cardiovasc Imaging 2017 10(10):1103-12.
3. Robson PM, Trivieri MG, Karakatsanis NK et al 2018, Phys. Med. Biol. https://doi.org/10.1088/1361-6560/aaea97
4. Grimm R, Furst S, Dregely I, et al. Self-gated radial MRI for respiratory motion compensation on hybrid PET/MR systems. Med Image Comput Comput Assist Interv 2013;16:17-24.
5. Fessler J et al. Image reconstruction toolbox, University of Michigan (https://web.eecs.umich.edu/~fessler/code/index.html).
6. Buerger C, Schaeffter T, King AP et al. Hierarchical adaptive local affine registration for fast and robust respiratory motion estimation. Medical Image Analysis, 15:551-564, 2011.
Figures