2183
Early Assessment of Subclinical Cardiac Involvement in Immune-Mediated Myopathy: a 3T Cardiac Magnetic Resonance Study1Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, P.R. China., China, 2Department of Radiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China, 3Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, wuhan, China, 4MR Collaboration, Siemens Healthcare, Ltd., Shanghai, P.R. China, shanghai, China, 5Tongji Hospital, Tongji Medical College, Huazhong, Wuhan, China
Synopsis
Cardiac involvement in immune-mediated myopathy often leads to a poor prognosis. We studied 32 patients with immune-mediated myopathies to investigate the role of cardiac magnetic resonance in the early detection of cardiac involvement. A comprehensive CMR examination using a 3T MR scanner, including the sequences for cardiac cine, T1 mapping (before and after contrast), T2 mapping, and late gadolinium enhancement (LGE), was performed on all the subjects. Focal myocardial fibrosis and diffusely elevated myocardial T1, T2, and ECV values were observed. The sequence of LGE combined with mapping technologies could improve sensitivity for the diagnosis of subclinical cardiac involvement.
Synopsis
Cardiac involvement in immune-mediated myopathy often leads to a poor prognosis. We studied 32 patients with immune-mediated myopathies to investigate the role of cardiac magnetic resonance in the early detection of cardiac involvement. A comprehensive CMR examination using a 3T MR scanner, including the sequences for cardiac cine, T1 mapping (before and after contrast), T2 mapping, and late gadolinium enhancement (LGE), was performed on all the subjects. Focal myocardial fibrosis and diffusely elevated myocardial T1, T2, and ECV values were observed. The sequence of LGE combined with mapping technologies could improve sensitivity for the diagnosis of subclinical cardiac involvement.Introduction
Immune-mediated myopathies (IMMs) are a group of heterogeneous muscle diseases, with a prevalence of 15 to 32 cases per 100,000. Cardiac damage in IMMs has been reported more frequently in recent years, and it is often subclinical and overlooked by clinicians. Unfortunately, cardiac involvement often leads to a poor prognosis [1]. In this study, we aimed to evaluate subclinical cardiac involvement in patients with IMM by using Cardiac Magnetic Resonance (CMR).Methods
A total of 32 patients with IMM and fifteen healthy controls were recruited into our study. The patients were divided into two groups based on whether a 12-lead ECG was abnormal. Fifteen patients with an abnormal 12-lead ECG and seventeen patients with normal ECG underwent a medical-history and laboratory examination. A comprehensive CMR examination using a 3T MR scanner (MAGNETOM Skyra, Siemens, Healthcare, Erlangen, Germany) was performed on all subjects. The CMR scan protocol included: cardiac cine, T1 mapping (before and after contrast), T2 mapping, and late gadolinium enhancement (LGE). The cardiac cine imaging parameters were as follows: slice thickness, 6 mm; slices: 6 - 8; TR: 25.12 ms; TE: 1.39 ms; flip angle, 55°; and the field of view was adjusted according to the patient's size. The LGE imaging parameters were as follows: TE, 1.1 ms; TR, 4.0 ms;flip angle, 20°;slice thickness, 6 mm; reconstructed matrix size, 256 *192; and the inversion time was individually adjusted and aimed to complete nulling of the myocardium. The MOLLI sequence parameters were as follows: TE, 1.2 ms;flip angle, 35°; slice thickness, 5 mm; reconstructed matrix size, 256* 256 pixels; and with a 5b(3b)3b/4b(1b)3b(1b)2b scan scheme for pre- and post-contrast T1 before and 15–20 min after the administration of a contrast agent dose.Results
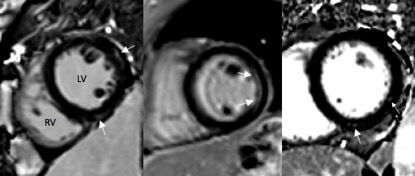
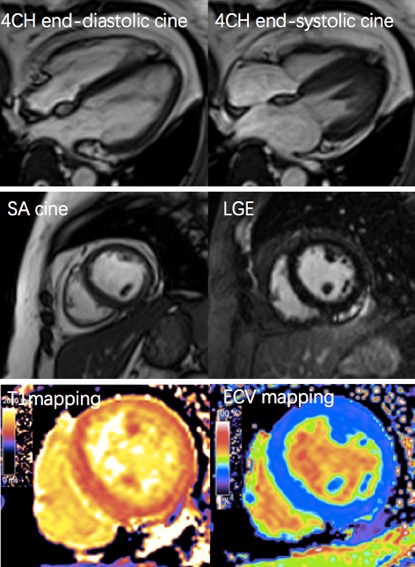
Focal myocardial fibrosis was found in 9/32 (28%) patients, most of which was located in the free wall of the left ventricle (LV). Among the 28% patients, six had a normal ECG. Focal fibrosis could occur in the epi-, mid-, and endomyocardium (Figure 1). In addition, the T1, T2, and ECV values of the interventricular septum in the middle segment were higher in IMMs than that in the controls, even in the patients who had no focal myocardial fibrosis (abnormal ECG), as shown in Figure 2. Elevated myocardium T1 values, T2 values, and extracellular volume (ECV) fractions of the LV were evident both in patients with LGE and patients without (both patients with abnormal ECGs and patients without) compared with the controls (p < 0.05).Discussion
The principal findings from this study indicated the following: 1) Normal ECG findings were not able to rule out the presence of focal myocardial fibrosis; 2) The combined application of the new CMR technology could improve the specificity for the diagnosis of heart involvement. According to our results, we found that the LV free wall was more susceptible, consistent with autopsy reports [2]. The increased T1, T2 and ECV values in IMMs might be caused by diffuse lesions such as myocardial inflammatory infiltrates or diffuse fibrosis, in view of the following arguments. First, myocarditis is one of the pathological mechanisms underlying IMM. Inflammatory myocardial infiltrates, like those detected in skeletal muscle, have been described in IMM patients [3]. Second, the application of mapping technology, reported in myocarditis and other cardiomyopathies, contributes to the non-invasive characterization of histological changes such as myocardial edema and fibrosis [4-8]. We showed that the sequence of LGE combined with mapping technologies could improve the sensitivity for the diagnosis of subclinical cardiac involvement.Conclusion
A combination of mapping technique and LGE sequence in CMR imaging can detect early subclinical cardiac involvement (such as focal and / or diffuse fibrosis and silent myocarditis) and may provide valuable information for screening high-risk patients with cardiac involvement. We therefore highly recommend CMR as the best choice for early detection of heart abnormities in patients with immune-mediated myopathy.Acknowledgements
No acknowledgement found.References
1. Torres C, Belmonte R, Carmona L, Gómez-Reino FJ, Galindo M, Ramos B, Cabello A, Carreira PE. Survival, mortality and causes of death in inflammatory myopathies. Autoimmunity. 2006; 39: 205-15.
2. Anders HJ, Wanders A, Rihl M, Krüger K. Myocardial fibrosis in polymyositis. J Rheumatol. 1999; 26: 1840-2.
3. Haupt HM, Hutchins GM. The heart and cardiac conduction system in polymyositis dermatomyositis: a clinicopathologic study of 16 autopsied patients. Am. J. Cardiol. 1982; 50: 998-1006.
4. Tessa C, Del Meglio J, Salvatori L, Casolo G. T1 and T2 mapping: new perspectives in cardiac magnetic resonance imaging. G Ital Cardiol (Rome). 2014; 15: 607-15.
5. Kellman P, Wilson JR, Xue H, Bandettini WP, Shanbhag SM, Druey KM, Ugander M, Arai AE. Extracellular volume fraction mapping in the myocardium, part 2: initial clinical experience. J Cardiovasc Magn Reson. 2012; 14:64
6. Ferreira VM, Piechnik SK, Dall'Armellina E, Karamitsos TD, Francis JM, Ntusi N, et al. T (1) mapping for the diagnosis of acute myocarditis using CMR: comparison to T2-weighted and late gadolinium enhanced imaging. JACC Cardiovasc Imaging. 2013; 6: 1048-1058.
7. Wassmuth R, Prothmann M, Utz W, Dieringer M, von Knobelsdorff-Brenkenhoff F, Greiser A, Schulz-Menger J. Variability and homogeneity of cardiovascular magnetic resonance myocardial T2-mapping in volunteers compared to patients with edema. J Cardiovasc Magn Reson.2013; 15: 27
8. Baeßler B, Schaarschmidt F, Dick A, Stehning C, Schnackenburg B, Michels G, Maintz D, Bunck AC. Mapping tissue inhomogeneity in acute myocarditis: a novel analytical approach to quantitative myocardial edema imaging by T2-mapping. J Cardiovasc Magn Reson. 2015; 17:115.
Figures