2175
Non-contrast, free-breathing pulmonary perfusion imaging in pediatric patients with congenital heart disease using multi-slice FAIR at 1.5T1Pediatrics, UT Southwestern Medical Center, Dallas, TX, United States, 2Radiology, UT Southwestern Medical Center, Dallas, TX, United States, 3Advanced Imaging Research Center, UT Southwestern Medical Center, Dallas, TX, United States
Synopsis
Congenital heart disease (CHD) is associated with anatomical abnormalities in the pulmonary arteries (PAs) which can result in asymmetric flow to the lungs, as well as an overall reduction in lung perfusion. Non-contrast pulmonary perfusion imaging using arterial spin labeling has the potential to provide both quantitative perfusion maps as well as a measure of asymmetric pulmonary blood flow. In this study, multi-slice, free-breathing pulmonary perfusion imaging is demonstrated using the FAIR technique for full coverage of the lungs, and flow measurements are compared with the standard phase contrast measurement approach.
Introduction
Congenital heart disease (CHD) is associated with anatomical abnormalities in the pulmonary arteries (PAs) which can result in asymmetric flow to the lungs, as well as an overall reduction in lung perfusion. Clinical evaluation of patients with the potential for asymmetric pulmonary flow is currently performed using phase contrast MRI. However, pulmonary perfusion imaging has the potential to provide a measure of flow distribution, as well as regional maps of quantitative perfusion. Arterial spin labeling (ASL) is a non-contrast perfusion MRI technique that can be used to generate quantitative perfusion maps, making it ideal for CHD patients needing longitudinal monitoring and for those with contraindications to contrast administration. Although ASL has been widely applied for pulmonary perfusion imaging in adults [1-3], studies in pediatric populations are limited [4]. The purpose of this study was: 1) to demonstrate the feasibility of whole-lung perfusion imaging using ASL in pediatric populations with CHD, 2) to compare the resulting perfusion measurements with the established phase-contrast technique, and 3) to assess the ability of optimized background suppression (BGS) to reduce motion artifacts to enable robust quantitative perfusion mapping during free-breathing.Methods
Nine patients with CHD (11 ± 7 years old; Figure 1), were scanned on a 1.5T Philips Ingenia with IRB approval and informed assent. Sagittal multi-slice flow alternating inversion recovery (MS-FAIR) [2] perfusion images were acquired across both lungs in each patient. The sequence began with saturation of the imaging region, followed by labeling with a pair of selective and non-selective inversions using a hyperbolic secant pulse. A post-labeling delay of one cardiac cycle (R-R interval) [1] was used to allow labeled blood to perfuse the lungs. A SShTSE acquisition was used to minimize the susceptibility artifacts due to B0 inhomogeneities in the lungs. The sequence was ECG-triggered to place the acquisition during the diastolic phase of the following cardiac cycle. BGS was applied using four non-selective inversion pulses during the inversion time [5]. FOCI inversion pulses were used for improved suppression in regions of B0 and B1 inhomogeneities [3, 6]. Although FAIR perfusion images are regularly acquired during guided breathing or an extended breathhold, these approaches can be difficult for some pediatric patients. Because BGS has been shown to significantly reduce respiratory motion artifacts near the diaphragm [3], a free breathing approach was used in this study for patient comfort, and to evaluate the resulting image quality in the presence of uncontrolled respiratory motion. 5-8 slices were acquired to cover an entire lung with 3 signal averages over 1.5 minutes of free breathing. The slice thickness was 15mm and resolution = 3x3 mm2. A separate M0 image was acquired for quantification [2, 7]. To measure true tissue perfusion, pooled blood in the major pulmonary vasculature was masked prior to measuring average perfusion across all slices [2]. Images were reconstructed and segmented offline in MATLAB. As part of the clinical protocol, phase contrast measurements were made in the branch PAs to assess differential pulmonary blood flow [8]. Both the flow ratio between lungs, as well as flow rate in the PAs were correlated with FAIR measurements in each lung.Results
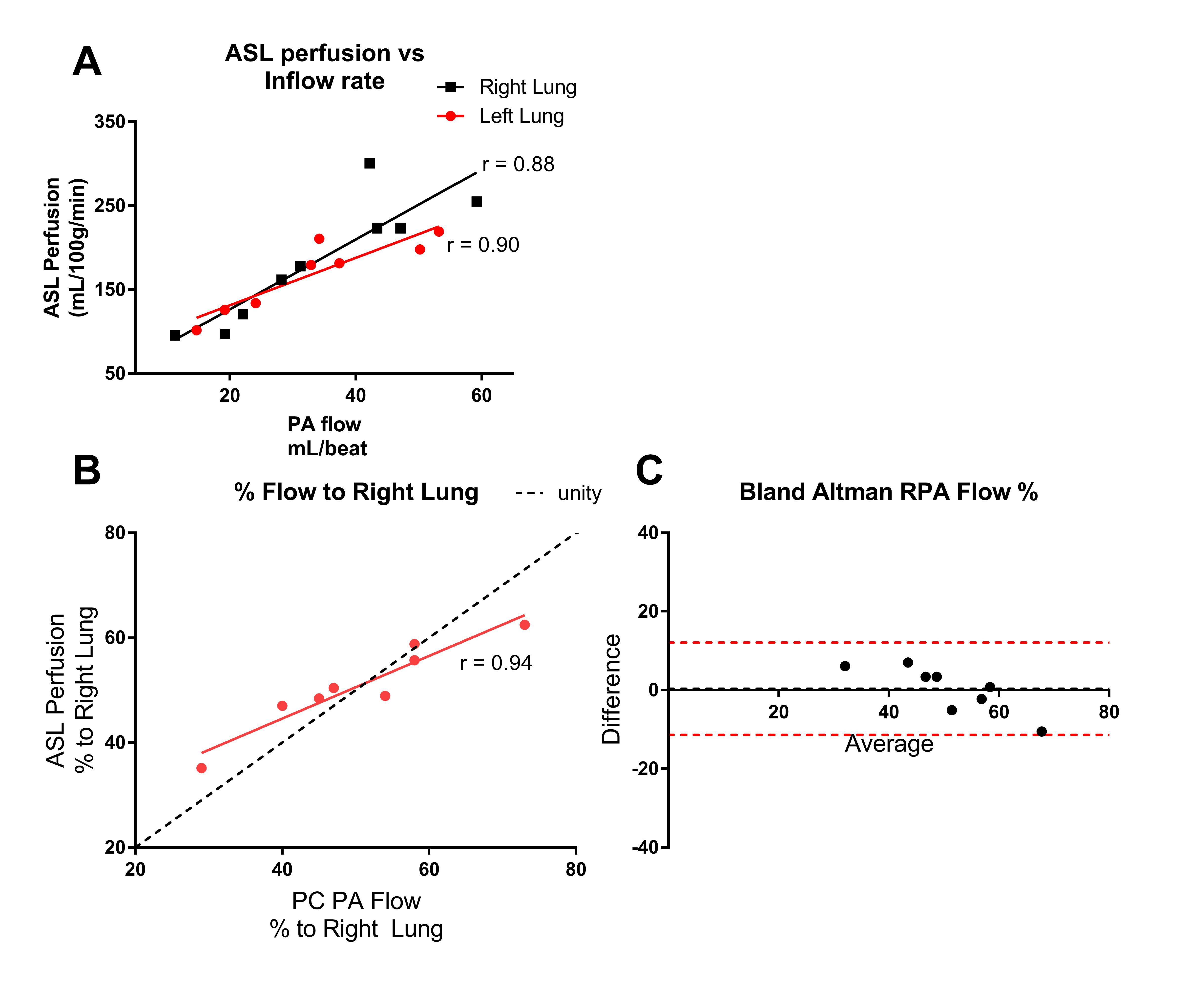
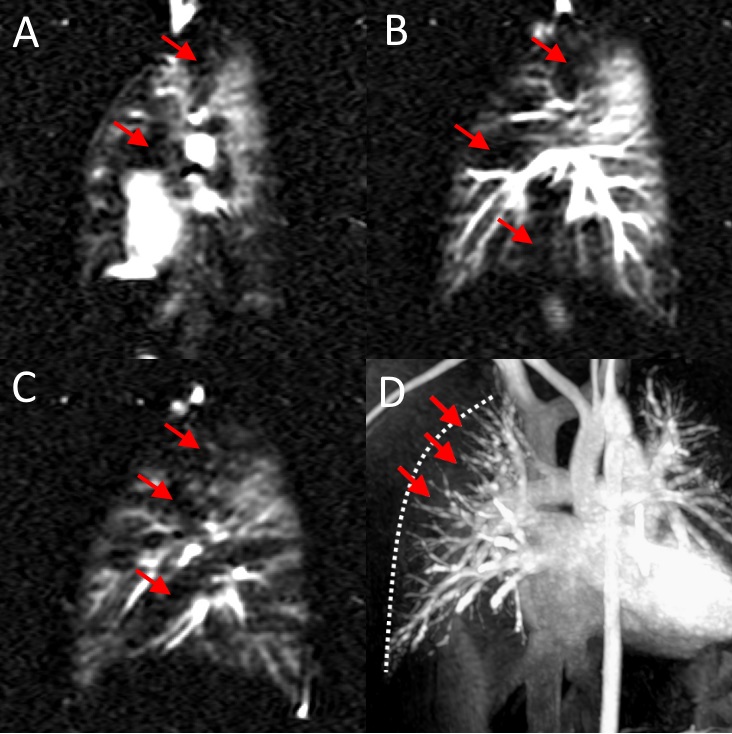
Figure 2 shows representative MS-FAIR perfusion images across both lungs in one patient. BGS enabled the patients to breathe freely throughout all perfusion scanning without introducing misregistration artifacts at the chest wall or diaphragm. Figure 3 (A) shows excellent agreement between quantified perfusion and the flow rate through the PAs to each lung, and (B,C) show excellent agreement between the left/right flow ratio between phase contrast and ASL. Figure 4 shows quantified perfusion maps across the lungs in two patients, showing good agreement with the flow per heartbeat in the right and left PAs. The average perfusion across all subjects was 183±72 and 168±42 mL/100g/min in the right and left lungs. Figure 5 shows one patient that also had pulmonary hypertension. The FAIR technique was able to detect patches of perfusion deficits that are characteristic of pulmonary hypertension. A contrast-enhanced angiography (Fig. 5D) scan also showed the expected peripheral pulmonary vascular pruning that occurs in these patients, leading to reduced pulmonary perfusion.Discussion
MS-FAIR with BGS enabled whole-lung coverage during free-breathing in a clinically acceptable scan time. Quantified perfusion measurements in the lungs agreed well with the established phase contrast approach, although the average perfusion was markedly lower than the expected perfusion in adults (400-600 mL/100g/min) [1, 2]. Future improvements to this technique will include reducing bright signal in the pulmonary vasculature to enable evaluation of the underlying perfusion using inflow saturation during the end of the inversion time [3].Acknowledgements
No acknowledgement found.References
[1] D. S. Bolar et al., "Quantification of regional pulmonary blood flow using ASL-FAIRER," Magn Reson Med, vol. 55, no. 6, pp. 1308-17, Jun 2006.
[2] J. S. Greer et al., "Non-contrast quantitative pulmonary perfusion using flow alternating inversion recovery at 3 T: A preliminary study," Magnetic resonance imaging, vol. 46, pp. 106-113, 2018.
[3] J. S. Greer, X. Wang, and A. J. Madhuranthakam, "Robust non-contrast perfusion imaging of whole-lungs using multi-slice FAIR at 3T," in International Society for Magnetic Resonance in Medicine, Paris, France, 2018, p. 2178.
[4] M. C. Liszewski et al., "Magnetic resonance imaging of pediatric lung parenchyma, airways, vasculature, ventilation, and perfusion: state of the art," Radiologic Clinics, vol. 51, no. 4, pp. 555-582, 2013.
[5] N. Maleki, W. Dai, and D. C. Alsop, "Optimization of background suppression for arterial spin labeling perfusion imaging," MAGMA, vol. 25, no. 2, pp. 127-33, Apr 2012.
[6] X. Wang et al., "Frequency Offset Corrected Inversion Pulse for B0 and B1 Insensitive Fat Suppression at 3T: Application to MR Neurography of Brachial Plexus," Journal of Magnetic Resonance Imaging, vol. 48, no. 4, pp. 1104-1111, 2018.
[7] R. B. Buxton et al., "A general kinetic model for quantitative perfusion imaging with arterial spin labeling," Magnetic resonance in medicine, vol. 40, no. 3, pp. 383-396, 1998.
[8] S. Sridharan, G. Derrick, J. Deanfield, and A. Taylor, "Assessment of differential branch pulmonary blood flow: a comparative study of phase contrast magnetic resonance imaging and radionuclide lung perfusion imaging," Heart, vol. 92, no. 7, pp. 963-968, 2006.
Figures