2168
Assessment of regional ventricular function in tetralogy of Fallot using strain analysis. Comparison of techniques1Medical College of Wisconsin, Milwaukee, WI, United States, 2University of Michigan, Ann Arbor, MI, United States
Synopsis
Assessment of ventricular function, especially in the right ventricle (RV), is important for cardiac evaluation in Tetralogy of Fallot (ToF). MRI tissue tracking (TT) is a recently introduced technique for analyzing myocardial strain directly from the cine images. In this study, we evaluate the feasibility of using TT strain analysis for measuring myocardial contractility in ToF and compare the results to measurements from the more established strain-encoding (SENC) MRI technique. The results showed that TT strain analysis allows for fast assessment of heart contractility in ToF with global strain measurements that are insignificantly different from those from SENC analysis.
INTRODUCTION
Assessment of ventricular function, especially in the right ventricle (RV), is a key factor for decision making in Tetralogy of Fallot (ToF) [1]. In this respect, MRI has been shown to be a valuable tool for evaluating ventricular function [2,3].
Although ejection fraction (EF) provides a good idea about global ventricular function, it may not be sensitive enough for detecting subtle ventricular function changes, especially in repaired ToF. In this respect, measures of regional heart mechanics, e.g. myocardial strain, are more suitable for accurate and early detection of changes in heart function, and have been shown to predict quality of life in repaired ToF [4].
Tissue tracking (TT) is a recently introduced technique for analyzing myocardial strain directly from the cine images without the need for additional tagging acquisition [5]. MRI TT has been mainly used for measuring global myocardial deformation and providing general information about heart contractility.
MRI strain-encoding (SENC) is a more established technique for measuring tissue deformation, which has a number of advantages [6]. It is fast and can be implemented as a single-heartbeat free-breathing acquisition with reasonable image quality. SENC can be acquired with high spatial resolution on the pixel level, and post-processing is simple and fast, resulting in a color-coded strain maps obtained from the acquired images.
In this study, we evaluate the feasibility of using MRI TT strain analysis for measuring myocardial contractility in ToF and compare the results to measurements from SENC analysis.
METHODS
This HIPAA compliant study was approved by our Institutional Review Board, and informed consent was obtained from all participants. Ten ToF patients (m/f = 4/6 and age = 42±22 y.o) were imaged on a 1.5T Philips MRI scanner. The MRI exam included the following: 1) cine imaging: long-axis (LAX) and a stack of short-axis (SAX) images covering the heart; 2) phase-contrast (PC) flow imaging through large arteries and atrioventricular valves; and 3) SENC imaging: base, mid, and apical SAX images and one 4-chamber image.
The cine images were analyzed to measure ejection fraction (EF) and myocardial circumferential (Ecc), longitudinal (Ell), and radial (Err) strains (using the tissue tracking (TT) technique). The PC images were analyzed to measure pulmonary-to-systematic flow ratio (Qp/Qs) and valvular regurgitations. The SENC images were analyzed to measure regional strain (Ecc and Ell) as a reference for TT measurements.
Statistical t-test and correlation analyses were conducted to measure differences in strain measurements between different techniques and the correlation between strain and EF, respectively (p<.001 considered significant).
RESULTS
Two patients showed residual ventricular septal defects (Qp/Qs = 1.6 and 1.2), six patients showed mild RV hypertrophy (mass-to-volume ratio = 0.2-0.25), six patients showed RV dilation (indexed EDV = 138±20 mL/m2), and nine patients showed both tricuspid regurgitation (12.4±6.4%) and pulmonary regurgitation (26.1±16%).
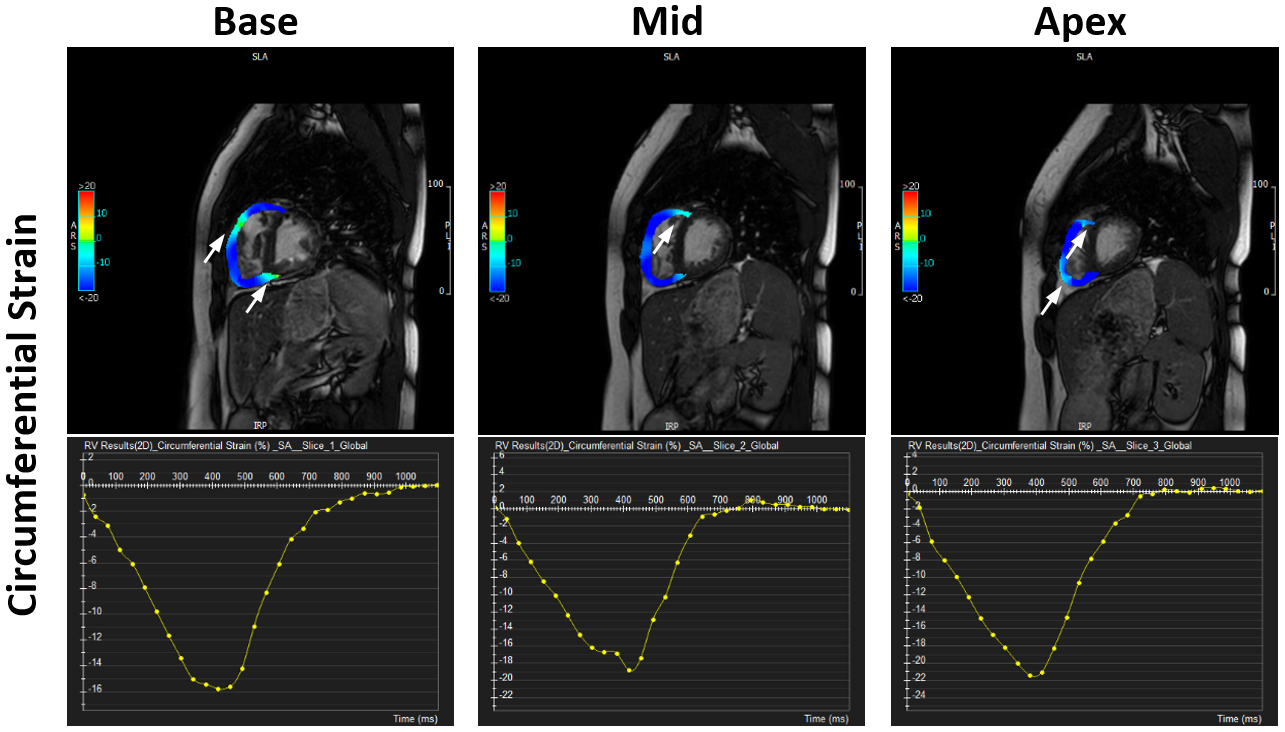
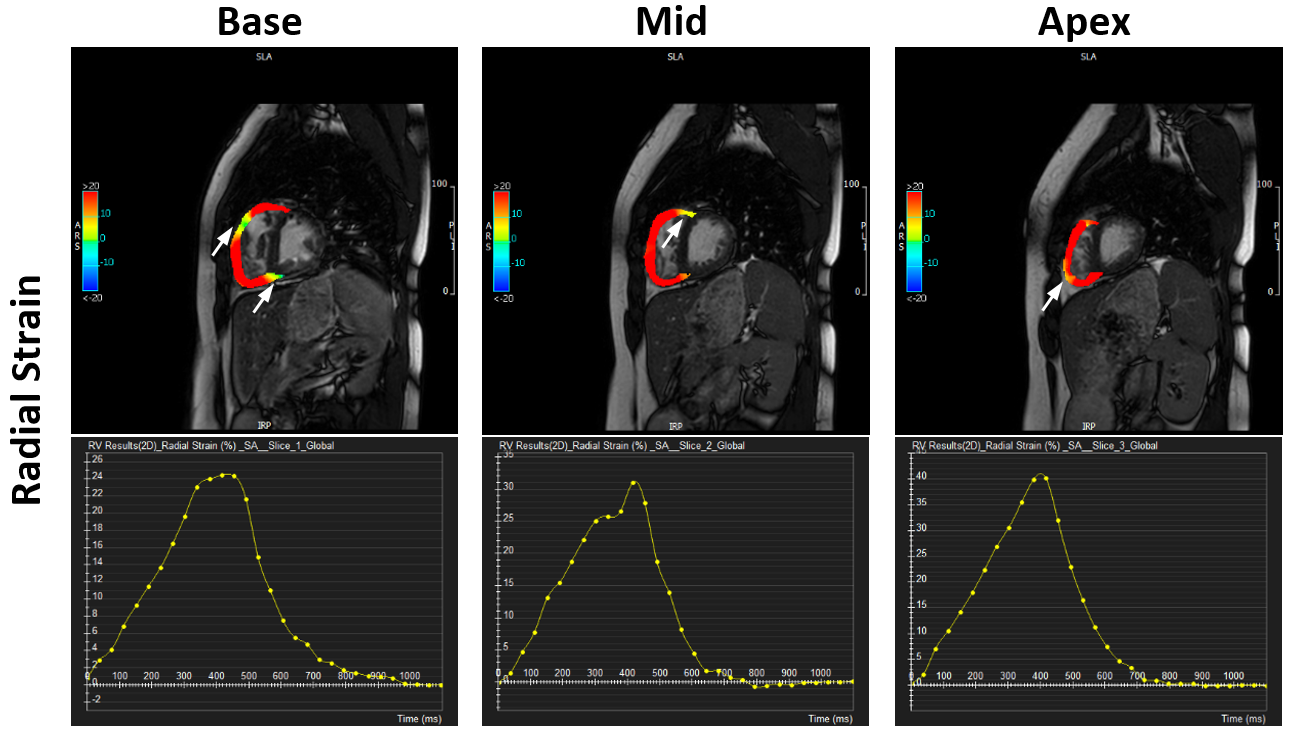
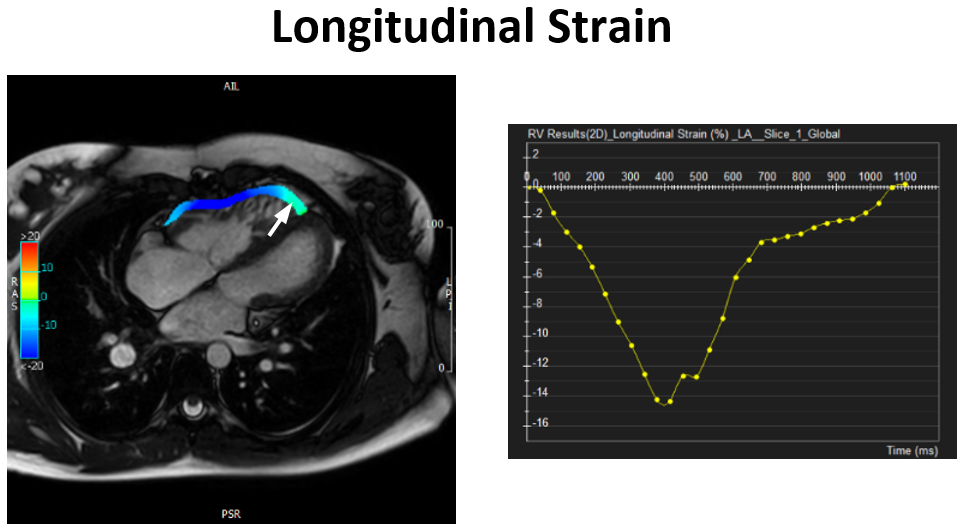
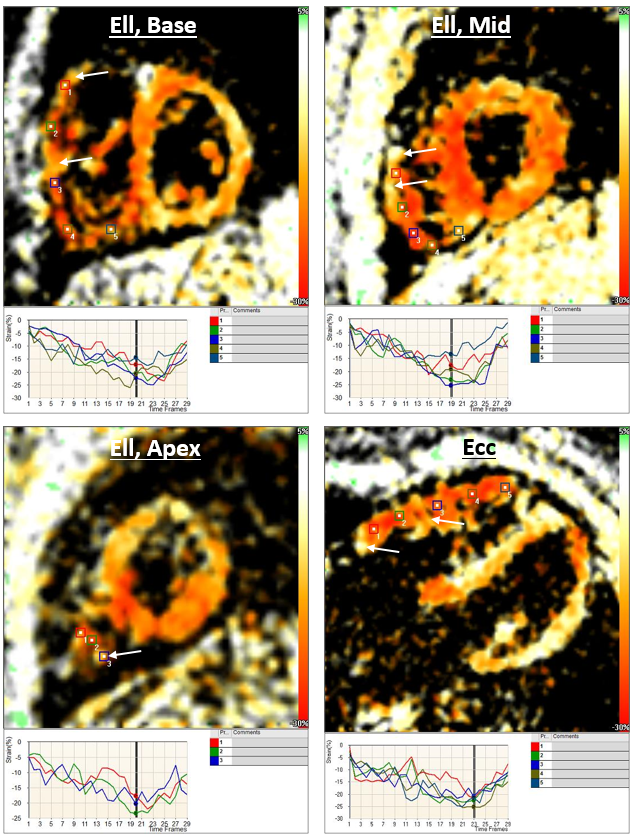
Figures 1-4 show RV strain results in the same patients using TT and SENC analysis. RVEF was 46±6% and TT (SENC) RV strain measurements were as follows: Ell = -21.2±5.5% (-20.2±2.9), Ecc = -21±2.6% (-15.7±6.3%), and Err = 43.8±14.9%. TT measurements did not show significant differences compared to SENC (p = .5 and .01 for RV Ell and Ecc, respectively). Strain showed weak correlation with RVEF (r(p) = 0.36(.3), 0.3(.4), and 0.12(.7) for Ecc, Err, and Ell, respectively).
LVEF was 55.2±8.5% and TT (SENC) LV strain measurements were as follows: Ell = -18.9±3.1% (-21.7±3.7), Ecc = -23.6±3.3% (-18.3±4.7), and Err = 50.8±17.1%. TT measurements did not show significant differences compared to SENC (p = .2 and .005 for LV Ell and Ecc, respectively). Strain showed strong correlation with LVEF (r(p) = 0.83(.002), 0.79(.006), and 0.86(.001) for Ecc, Err, and Ell, respectively).
DISCUSSION and CONCLUSION
Despite acceptable LVEF and borderline RVEF in most patients, results showed depressed strain, especially in the RV. TT strain measurements showed insignificant differences compared to SENC, where the largest differences occurred in Ecc measurements, especially in the RV. This could be interpreted by the heterogeneous strain pattern observed in the SENC images (Figure 4), secondary to the SENC high resolution capability versus the global nature of strain measurement in TT. The weak correlation between strain and EF in the RV, compared to the LV, can be interpreted by the major effect of ToF on RV function, which is more elicited by analyzing heart mechanics, in addition to EF measurement, for better understanding and early detection of cardiac dysfunction in ToF.
In conclusion, TT strain analysis allows for fast assessment of heart contractility in ToF with global strain, especially Ell, measurements that are insignificantly different from those from SENC analysis.
Acknowledgements
No acknowledgement found.References
1. Khalaf et al, Ped Card 34:1206-1211
2. Samyn et al, J Magn Reson Imaging 26:934-940
3. Jing et al, Eur Heart J CVI 15:1333-1143
4. Ibrahim. Heart mechanics MRI. CRC Press, 2017
5. Padyiath et al, Echocardiography 30:203-10
6. Osman et al, Magn Reson Med 46:324-334
Figures