2167
Comparison of Different Real-Time Sequences for Cardiac MRI1Department of Internal Medicine II, University Ulm Medical Center, Ulm, Germany, 2Core Facility Small Animal Imaging (CF-SANI), Ulm University, Ulm, Germany
Synopsis
In this work we compare different real-time protocols for cardiac functional imaging. Image quality is assessed qualitatively and quantitatively and functional parameters are calculated from three short axis slices. All imaging methods are compared to the current ECG-gated, breathhold reference standard (BH-CINE). All real-time methods show acceptable visual image quality with only slight differences, which is supported by the quantitative analysis. The functional analysis shows slight systematic differences, but not on a statistically significant level.
Introduction
Real-time (RT) approaches in cardiac magnetic resonance imaging (CMR) can be considered a global goal. They enable the assessment of function, volumes and structure based on data acquired during free-breathing and without ECG. Although the breathhold, ECG gated acquisition (BH-CINE) represents the current reference standard, image quality can suffer in cases of insufficient patient cooperation (breathhold) or in severe arrhythmia. Different RT imaging methods have been presented in recent years, mostly relying on non-cartesian k-space sampling in combination with Compressed Sensing1,2. In this work, the performance of radial and spiral tiny golden angle sequences and a novel sliding window reduced-FOV EPI technique3, enabling higher acceleration factors than pure parallel imaging, are compared against each other and the BH-CINE reference.Methods
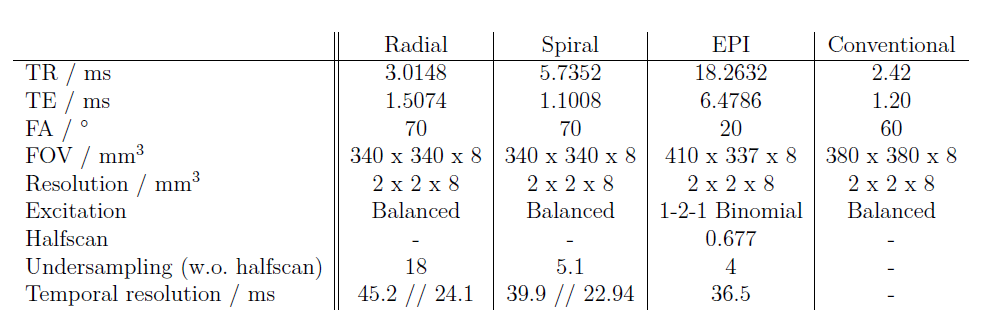
All imaging experiments were performed on a 1.5 T clinical whole-body scanner (Philips Achieva 1.5T, Best, The Netherlands) with a maximum gradient strength of 21 mT/m per channel and maximum slew rate of 180 T/m/s. All data were acquired with a 32-element SENSE cardiovascular array coil. Three volunteers (one with ventricular premature beats, unknown before this study) have undergone a standardized examination consisting of BH-CINE examination and the three real-time sequences in three short axis slices (basal, medial, and apical). The BH-CINE sequence is considered as the clinical standard. The radial b-SSFP sequence comprised a tiny golden angle (TyGA) trajectory4. The spiral sequence comprised an Archimedean spiral with a fixed acquisition time of 3 ms. The angle between consecutive interleaves was determined as a modified TyGA trajectory for center-out acquisitions (TyGA-CAT). All data were reconstructed by a k-t SPARSE-SENSE framework with a Total Variation (TV) sparsity operator. $$$k$$$-space coverage (a) and the principal workflow (b) of the sw-rFOV reconstruction are shown in figure 1. For image quality quantification the following properties were calculated:
- SNR (blood and myocardium, with SNR defined as mean signal divided by the standard error in the same region,
- CNR between myocardium and blood,
- edge sharpness derived from the mean value of a normalized, Sobel filtered fixed ROI encompassing the heart and an interpolated pixel distance for a chosen increase in signal (25% to 75% of the difference).
Further, functional parameters of the left ventricle were calculated with Segment (Medviso AB, Lund, Sweden).
Results
Exemplary end-diastolic images (a) from the reconstructed movies and m-mode representation (b) for one volunteer with ventricular premature beats are given in figure 2. Quantitative image analysis is shown in figure 3 and the functional parameters are given in table 2.Discussion
All imaging techniques showed diagnostic image quality for real-time acquisitions. In direct comparison, the spiral images showed the highest level of detail due to the efficient sampling scheme and corresponding lower undersampling factors. At the same time, the relatively long readout leads to swirling flow artifacts. In radial imaging, undersampling artifacts (in the form of streaks) are visually most prominent, although not altering the region of interest. The SNR of myocardium is highest for sw-rFOV reconstructed images, in the blood pool SNR is in the same range for all acquisitions. Compared to the CS reconstructed non-cartesian images, the sw-rFOV images exhibit decreased CNR, most likely due to the different sequence scheme (non-balanced). The sharpness metrics have to be considered with caution, e.g. double edges or streaking artifacts can lead to high values in the sobel edge index. However, the results are mostly in line with the expectation. The signal increase is best for rFOV imaging (having the highest temporal resolution), the sobel edge index is best for radial imaging, as the contrast behavior in combination with the short readouts lead to a clear depiction of epicardium. For the deviation of the functional values compared to the reference standard, it should be kept in mind that real-time approaches are acquired during free breathing. This could lead to a slight displacement of the imaged slice.
Although a Wilcoxon test did not show significance of the differences, the deviations seen in the data can be explained: While stroke volume and ejection fraction appear most stable, the lower value of the end-systolic volume for the real-time approaches can be explained by the high temporal resolution in EPI and the flexibility in the sliding window reconstruction of the non-cartesian sequences.
Conclusion
All presented approaches show promising results for RT cardiac imaging. The different image quality metrics cannot determine a single “best” method but are in line with theoretical expectations. Functional parameters show good accordance with the reference standard. Further examinations in a larger cohort are necessary to validate a feasible RT functional imaging protocol.Acknowledgements
The authors thank the Ulm University Centre for Translational Imaging MoMAN for its support.References
(1) Steeden, J. A., Kowalik, G. T., Tann, O., Hughes, M., Mortensen, K. H., & Muthurangu, V. (2018). "Real-time Assessment of Right and Left Ventricular Volumes and Function in Children Using High Spatiotemporal Resolution Spiral bSSFP with Compressed Sensing." arXiv preprint arXiv:1804.09480.
(2) Feng, X., Salerno, M., Kramer, C. M., & Meyer, C. H. (2016). "Non‐Cartesian balanced steady‐state free precession pulse sequences for real‐time cardiac MRI." Magnetic resonance in medicine, 75(4), 1546-1555.
(3) Metze, P., Speidel, T., Stumpf, K., Rasche, V. "Sliding Window Reduced FOV Reconstruction in EPI for Real-Time Cardiac Imaging." Submitted to this conference
(4) Wundrak, Stefan, et al. "Golden ratio sparse MRI using tiny golden angles." Magnetic resonance in medicine 75.6 (2016): 2372-2378.
Figures