2161
Robust free-breathing cardiac cine-MRI using a combination of serial motion averaging and Compressed SENSE1Department of Radioligical Services, Tokyo Women's Medical University Hospital, Tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Tokyo Women's Medical University Hospital, Tokyo, Japan, 3Philips Japan, Tokyo, Japan
Synopsis
The present study investigates the clinical utility of cardiac cine-MRI using free-breathing scan with serial motion averaging (SMART) and Compressed-SENSE (C-SENSE). Left ventricular functional parameters derived from free-breathing SMART with C-SENSE showed good correlations to those from conventional breath-hold technique. Cine-MRI with C-SENSE can reduce both scan time (around 40% of the scan time) and burden of multiple breath-holdings without any penalty for the image quality; therefore, it might contribute to great advantages in routine clinical work.
Purpose
Cardiac cine-MRI is used as a standard method for ventricular volumetric analyses (1). Basically, whole-heart cine-MRI requires multiple time of breath-holding; hence it is often challenging to examine children and elder patients. To solve this problem, free-breathing scan with serial motion artifact reduction technique (SMART) has been often used, but SMART requires long acquisition time (i.e., multiple number of signal averages:NSAs) for effectively reducing motion artifacts by using long term averaging (2). Recently, a hybrid technique of compressed sensing and SENSE (Compressed SENSE: C-SENSE) has been developed to shorten scan time while maintaining the image quality (3,4). The present study investigates the clinical utility of cardiac cine-MRI using free-breathing scan using a combination of SMART and C-SENSE by comparing conventional breath-holding scan and free-breathing SMART scans.
Methods
[Subjects] Cardiac cine-MRI imageswith ten healthy volunteers (eight male and two female, age range: 25-42 years) were obtained by 3.0T MR system (Ingenia, Philips healthcare). We compared three types of cine images: conventional breath-hold technique, free-breathing SMART, and free-breath SMART with C-SENSE (Fig. 1). We evaluated the reproducibility of left ventricular functional parameters (left ventricular ejection fraction, LVEF %; left ventricular end-diastolic volume, LVEDV ml; and left ventricular end-systolic volume, LVESV ml) among three methods. Functional analysis was performed by one radiologist and one technologist using available software (Ziostation 2, Ziosoft Co, Tokyo). [Cardiac cine-MRI] Image parameters: cardiac synchronization=retrospective, slice thickness=8mm, FOV 320mm, NSA=1, pixel size=1.25X1.26mm, TR=3.5msec, TE=1.5msec, FA=45deg, number of heart phase=20. [Statistical analysis] Correlation of parameters was analyzed by Linear regression analysis and Bland-Altman plot analysis. Probability values <0.05 were considered as significance.
Results & Discussion
Excellent correlations in all three parameters (LVEF, LVEDV and LVESV) were obtained between breath-holding and free-breathing SMART (Fig. 2), and between breath-holding and free-breathing SMART with C-SENSE (Fig. 3). Bland-Altman regressions show a little unevenness in three parameters between breath-hold and free-breathing SMART (Fig. 4). On the other hand, the unevenness in LVEDV and LVESV between breath-holding and free-breathing SMART with C-SENSE became small (Fig. 5). The average scan time was 2 minutes 30 seconds for free-breathing SMART and 1 minute 30 seconds for free-breathing SMART with C-SENSE. Free-breath SMART with C-SENSE can shorten around 40% of the scan time compared with free-breathing SMART.
Conclusion
Cardiac functional measurements derived from free-breathing SMART with C-SENSE were excellently agreements with those from the standard free-breathing technique. Cine-MRI with C-SENSE can reduce both scan time and burden of multiple breath-holdings without any penalty for the image quality; therefore, it might contribute to great advantages in routine clinical work.
Acknowledgements
No acknowledgement found.
References
(1) Germain P, et al: Inter-study variability in left ventricular mass measurement. Comparison between M-modeechography and MRI. Eur Heart J 13:1011-9, 1992. (2) Seitz J, et al: Reduction of motion artifacts in magnetic resonance imaging of the neck andcervical spine by long-term averaging. Invest Radiol 35: 380-4,2000. (3) Lustig M, et al: Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn Reson Med 58:1182-95, 2007. (4) Liang D, et al: Accelerating SENSE using compressed sensing. Magn Reson Med 62: 1574-84, 2009.
Figures

Figure 1: Cine imaging of breath-holding, free-breathing SMART, and free-breath SMART with Compressed SENSE. Acquisition time was 10 times of 7 seconds breath-holding for standard breath-holding, 2 minutes 28 seconds for free-breathing SMART, and 1 minutes 32 seconds for free-breathing SMART with Compressed SENSE.
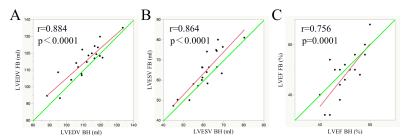
Figure 2: Linear regression analysis between standard breath-hold and free-breathing SMART.
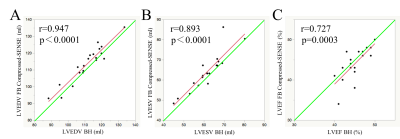
Figure 3: Linear regression analysis between standard breath-hold and free-breathing SMART with Compressed SENSE.
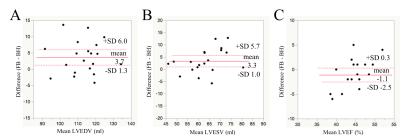
Figure 4: Bland-Altman plots between standard breath-hold and free-breathing SMART.
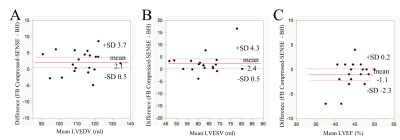
Figure 5: Bland-Altman plots between standard breath-hold and free-breathing SMART with Compressed SENSE.