2160
A preliminary study on the mechanism of left ventricular myocardial strain in patients with pulmonary hypertension1Department of Radiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, WUHAN, China, 2Department of Radiology, Wuhan General Hospital of Chinese People’s Liberation Army, WUHAN, China, 3MR Collaboration,Siemens Healthcare Ltd,Shanghai,China, SHANGHAI, China
Synopsis
There is little understanding
about the mechanism of left ventricular strain in pulmonary hypertension (PH)
patients at present. In this study, we compared left ventricular strain between
PH patients and the healthy controls. For PH patients with preserved or mildly improved
left ventricular ejection fraction (LVEF), the ventricular strain parameters decreased
compared to the healthy controls. We found that left ventricular myocardial
strain impairment in HP patients is associated with right ventricular overload
of volume or pressure and decreased ejection capacity.
Introduction
Left ventricular ejection fraction (LVEF) is considered to be an important clinical index of reflecting the ventricular function. However, for many pulmonary hypertension (PH) patients, the LVEF appears normal or, even mildly elevated. Myocardial strain, on the other hand, is more sensitive to the early ventricular deformation change[1]. At present, there is little understanding about the mechanism of left ventricular (LV) strain in PH patients. In this study, we aim to determine whether LV strain may be affected in PH patients, especially those with preserved or mildly improved LVEF and, whether chronic right heart failure affects regional LV function.Method
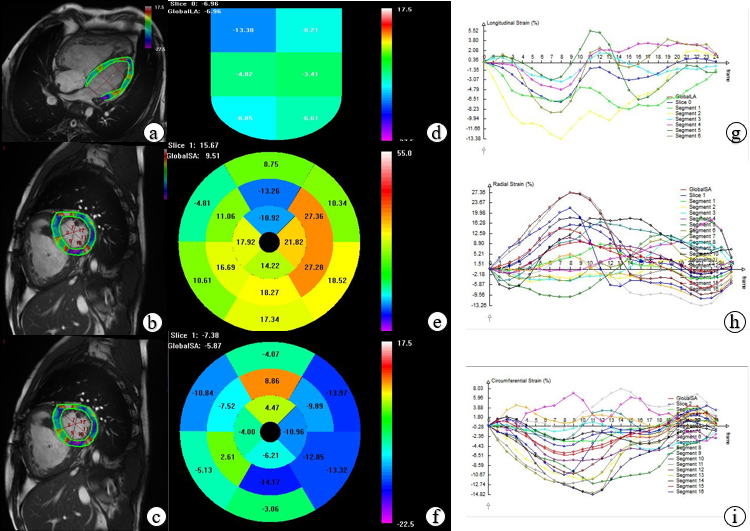
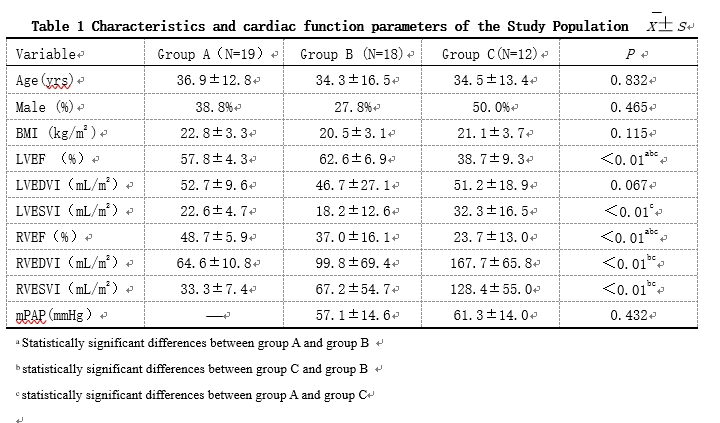
After informed consent, a total of 30 PH patients were evaluated with right heart catheterization (RHC) and cardiac magnetic resonance (CMR) imaging and were compared with 19 healthy volunteers. The presence of PH was defined as a mean pulmonary artery pressure >25 mm Hg at RHC. Patients with other LV disease unrelated to PH or ventricular shunt were excluded. All subjects were classified into: group A (healthy volunteers, LVEF ≥ 50%, N=19), group B (PH patients, LVEF ≥ 50%, N=18), and group C (PH patients, LVEF < 50%, N= 12). CMR studies were performed on two 1.5 Tesla MR scanners (MAGNETOM Aera or MAGNETOM Avanto; Siemens Healthcare, Erlanger, Germany) using a 18-channel phased-array body coil combined with the spine coil (12 of 36 channels used). Long-axis 4-chamber cine images and short-axis covering the whole heart cine images were obtained. Scan parameters for MAGNETOM Aera were: FOV = 340×255 mm2,acquisition matrix = 256×205,TR = 2.93 ms, TE = 1.16 ms,flip angle 80°,slice thickness = 6 mm; Scan parameters for MAGNETOM Avanto were: FOV = 360×288 mm2,acquisition matrix = 168×192, TR = 47.69 ms, TE = 1.08 ms, flip angle 65°, slice thickness = 8 mm. Cardiac function analysis was performed on a dedicated workstation (Argus, Siemens Medical Solutions, Erlangen, Germany) by manually outlining the endocardial contour of the left and right ventricles. LV and RV volumes were indexed to body surface area. Biventricular ejection fraction (EF), end-diastolic volume index (EDVI), end-systolic volume index (ESVI) were calculated. For the myocardial strain analyses, CMR cine images were loaded into a prototype post-processing software (TrufiStrain, version 2.0, Siemens Healthcare, Erlangen, Germany) to measure the global peak systolic longitudinal (Ell) strain, circumferential (Ecc) strain, and radial (Err) strain. Besides, LV regional Ecc and Err, including septum(AHA segments 2, 3, 8, 9, 14),lateral wall (AHA segments 5,6,11,12,16), anterior wall (AHA segments 1,7,13) and inferior wall(AHA segments 4,10,15)were measured on the short-axis cine images as well (Figure 1). Differences in two group were established using a 2-tailed unpaired Student t test, or in cases involving multiple groups, the ANOVA test and Kruskal Wallis test were used. Correlation between variables was assessed by Pearson or Spearman correlation coefficients.Result
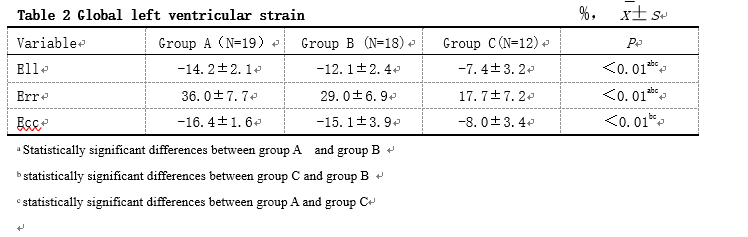
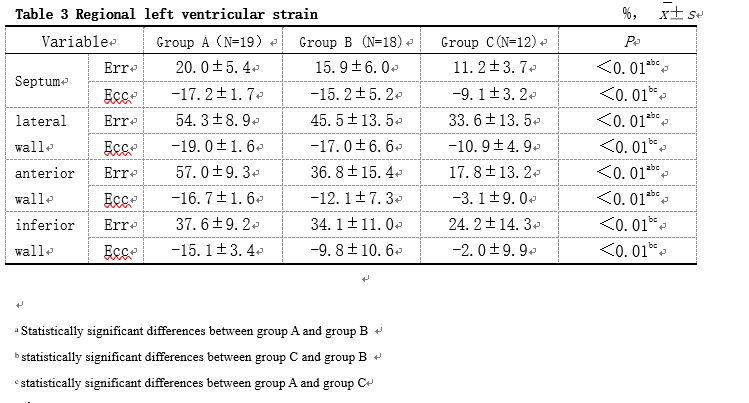
The global LV Ell and Err decreased in PH patients with preserved or mildly elevated LVEF, and all strain parameters decreased in PH patients with decreased LVEF (Table2 and 3). The regional LV Ecc was significantly associated with RVEDVI, especially in the septum (r = 0.732, P<0.01). The LV Err in the lateral wall was related to the mean pulmonary artery pressure (r = -0.419, P<0.05); and the global LV Err was significantly correlated with RVEF (r = 0.722, P<0.01).Discussion
The strain abnormality in patients with preserved or mildly elevated LVEF may be due to the fact that LVEF only reflects volume changes in LV and cannot reflect changes in myocardial ultrastructure associated with LV systolic function[2]. Ecc was significantly associated with RVEDVI, especially in the septum, which suggests that ventricular interdependence may be a potential etiology for abnormal LV function in PH patients[3]. when the right ventricular (RV) afterload is increased ,the ventricular septum bulges to the left side, so that the curve radius of the LV free wall and the tension are significantly higher than the ventricular septum, which may be the mechanism of decreased lateral Err caused by increased RV afterload. The RVEF is mainly the compression of the inner diameter between the free wall and the interventricular septum, and the power comes from the left ventricle. Increased RVEDV limits the LV filling and changes the shape and spatial structure of the left ventricle, making the left ventricle contraction does not continue to power the RV ejection ,which leads to further deterioration of RV function.Acknowledgements
No acknowledgement foundReferences
[1] Smiseth O A, Torp H, Opdahl A, et al. Myocardial strain imaging: how useful is it in clinical decision making?[J]. European heart journal, 2015, 37(15): 1196-1207.
[2] Tops L F, Delgado V, Marsan N A, et al. Myocardial strain to detect subtle left ventricular systolic dysfunction[J]. European journal of heart failure, 2017, 19(3): 307-313.
[3] Chungsomprasong P, Hamilton R, Luining W, et al. Left Ventricular Function in Children and Adolescents With Arrhythmogenic Right Ventricular Cardiomyopathy[J]. The American journal of cardiology, 2017, 119(5): 778-784.
Figures