2158
3D stack of spirals MRI with extra motion-state dimensions: a feasibility study1Institute of Cardiovascular Science, UCL, London, United Kingdom, 2Great Ormond Street Hospital for Children, London, United Kingdom
Synopsis
It has been previously shown that a 3D golden ratio stack of spirals sequence is suitable for fast thoracic MRI, including cardiac gated and elapsed time reconstructions. This work examines the feasibility of including a respiratory motion-state dimension. 5D thoracic datasets have been reconstructed using ESPIRiT to resolve along the cardiac and respiratory cycles. Although challenges exist, preliminary testing indicates that this is an effective method to increase data efficiency, thereby improving image quality and/or reducing the time of acquisition.
Introduction
In previous work, a golden ratio stack of spirals (GRASS) sequence was demonstrated to enable flexible reconstruction of angiographic data.1 However, respiratory navigation resulted in poor data efficiency. In this work, the concept of an extra respiratory dimension2 is applied to a 3D spiral sequence to increase data usage and reduce acquisition time.Methods
Acquisition: An RF-spoiled GRE pulse sequence developed in-house was used to acquire k-space data with a stack of spirals sampling pattern. The base trajectory, a uniform density spiral, was calculated using a publicly available numerical algorithm.3 This base spiral was then rotated within the kx-ky plane and translated along kz to cover a cylindrical k-space. Rotation angles and positions along kz were calculated using multidimensional golden means,4 which generalize the excellent sampling properties of the golden ratio to this two-dimensional problem. The following imaging protocol was used: flip angle = 15°, FOV = 400 x 400 x 150 mm3, matrix size = 256 x 256 x 96, which yields an isotropic voxel of size 1.6 x 1.6 x 1.6 mm3, number of spiral interleaves = 36. TR and TE were 9.36 ms and 1.64 ms, respectively. 3,080 points per readout were sampled at a bandwidth of 1,300 Hz/pixel. A total of 20,736 spiral interleaves were continuously acquired over 194 s, using 12 channels. ECG triggering was used for retrospective gating. All imaging was performed in a 1.5 T scanner (Siemens Avanto, Siemens Healthineers, Erlangen, Germany).
Data sorting: A respiratory self-navigation method was implemented based on the SI translation of body parts. SI projections were obtained by grouping the DC component (kx = ky = 0) of every readout in a sliding window fashion. These were then processed in the manner described by Pang et al.5 in order to bin data into different respiratory states. However, independent component analysis (ICA) was used rather than principal component analysis (PCA), as it was found to be more robust in our case. The cardiac data obtained by ICA was discarded as ECG data was available during the acquisition. Cardiac bins were populated according to each readout’s time point between ECG triggers. In order to perform a cardiac gated reconstruction, data were binned into 20 cardiac phases and 4 respiratory phases. Each bin had approximately 210 readouts, resulting in an acceleration factor of 16 and an acquisition efficiency of 81%.
Reconstruction: Images were reconstructed using the ESPIRiT method in the BART toolbox.6 Total variation was used as sparsifying transform along the cardiac and respiratory dimensions, with regularization values of 0.015 and 0.007, respectively. Sum-of-squares coil compression was used to reduce the quantity of data to 4 virtual channels. The computation was performed in the Google Cloud Platform, in an instance with 96 Skylake vCPUs and 624 GB of RAM. Reconstruction time was approximately 90 minutes. For comparison, a separate reconstruction was carried out without the respiratory dimension, instead using a 30% acceptance rate, which was chosen in line with previous work.1 This reconstruction was otherwise identical in terms of algorithm employed, number of cardiac phases, regularization values and number of iterations.
Results
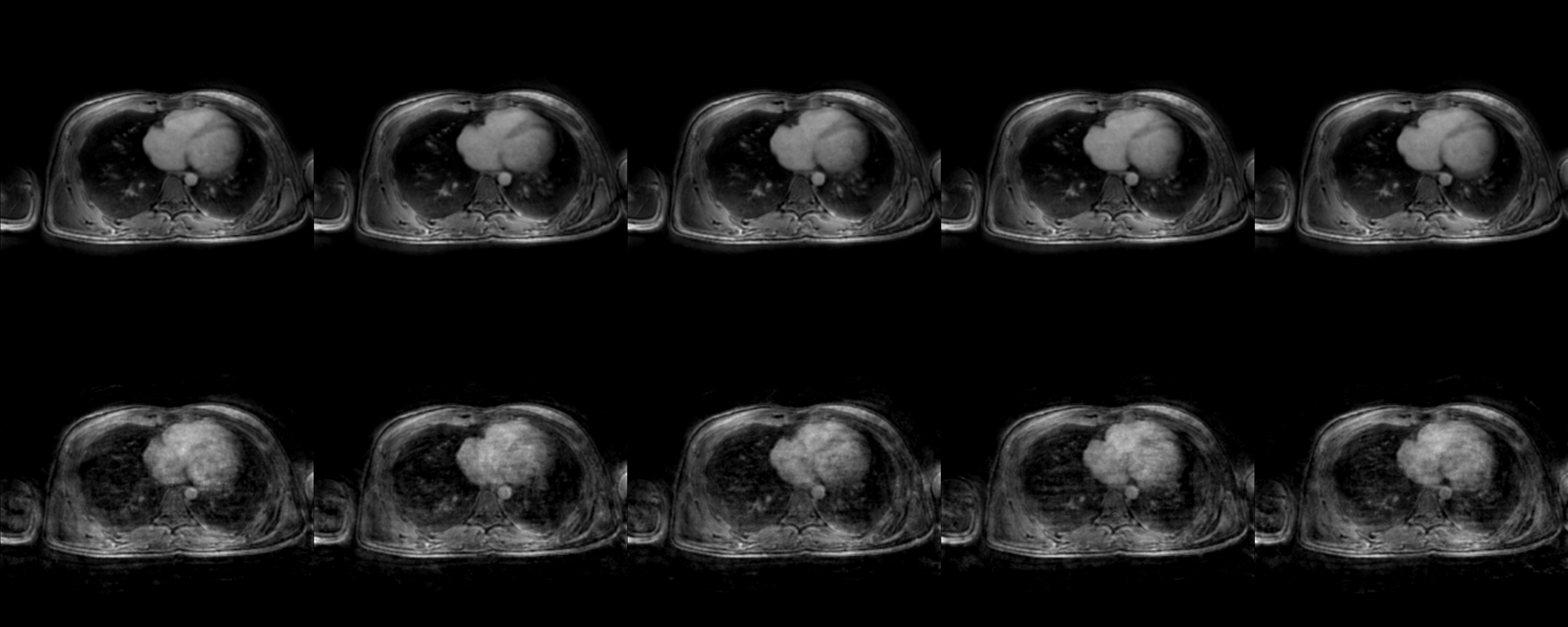
Figure 1 shows slices at different time points along the cardiac cycle, taken from a thoracic 5D dataset acquired and reconstructed as described above, as well as equivalent images for the control reconstruction. A reduction in undersampling artifacts is apparent in the new framework.Discussion
An extra respiratory dimension has been shown to successfully resolve respiratory motion, thereby reducing undersampling artifacts by exploiting sparsity along the respiratory dimension.2 This idea has been successfully applied to a stack of spirals sequence, enabling higher acceleration factors and improving data efficiency. In addition, it provides information on respiratory dynamics.
High computational requirements have been found to be a limiting factor. Although the resources needed are readily available in cloud platforms, they are expensive and sometimes impractical to use, especially as the size of the dataset grows (e.g. by increasing the matrix size). Further optimization in the implementation will be required to address this problem.
Conclusion
Preliminary tests indicate that an extra respiratory motion-state dimension can be incorporated into a stack of spirals sequence for fast 5D thoracic/abdominal MRI, and that it results in significant improvement in image quality and/or acquisition time.Acknowledgements
We would like to thank Heart Research UK for funding this research.References
1. Kowalik GT, Steeden JA, Atkinson D, Montalt-Tordera J, Mortensen KH, Muthurangu V. Golden ratio stack of spirals for flexible angiographic imaging: Proof of concept in congenital heart disease. Magnetic Resonance in Medicine. 2018;0(0):1-12.
2. Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magnetic Resonance in Medicine. 2016;75(2):775-788.
3. Pipe JG, Zwart NR. Spiral trajectory design: A flexible numerical algorithm and base analytical equations. Magnetic Resonance in Medicine. 2014;71(1):278-285.
4. Anderson PG. Multidimensional Golden Means. In: Bergum GE, Philippou AN, Horadam AF, eds. Applications of Fibonacci Numbers: Volume 5 Proceedings of ‘The Fifth International Conference on Fibonacci Numbers and Their Applications’, The University of St. Andrews, Scotland, July 20–July 24, 1992. Dordrecht: Springer Netherlands; 1993:1-9.
5. Pang J, Sharif B, Fan Z, et al. ECG and navigator-free four-dimensional whole-heart coronary MRA for simultaneous visualization of cardiac anatomy and function. Magnetic Resonance in Medicine. 2014;72(5):1208-1217.
6. Uecker M, Lai P, Murphy MJ, et al. ESPIRiT—an eigenvalue approach to autocalibrating parallel MRI: Where SENSE meets GRAPPA. Magnetic Resonance in Medicine. 2014;71(3):990-1001.
Figures