2156
Assessing the effects of substrate modulation on cardiac function and metabolism in the rodent heart with CINE MRI and hyperpolarized [1-13C]pyruvate1Department of Physiology Anatomy and Genetics, University of Oxford, Oxford, United Kingdom, 2John Radcliffe Hospital, Oxford Centre for Magnetic Resonance, Oxford, United Kingdom
Synopsis
Heart failure is associated with reduced cardiac energetics and this has been linked to impaired substrate utilization. We have assessed in rats how cardiac function and pyruvate dehydrogenase (PDH) flux change upon substrate manipulation, by varying plasma non-esterified fatty acid (NEFA) levels with acipimox injections in both fed and fasted rats. We found that NEFA depletion in fasted rats led to cardiac systolic dysfunction which may be explained by an insufficient compensatory increase in PDH flux boosting glucose oxidation. This model of substrate-manipulation heart failure could be used to assess potential heart-failure drugs in the future.
Purpose
Heart failure is a leading cause of death world-wide and the underlying pathology is characterized by changes in cardiac metabolism and energetics1. The healthy heart relies on fatty acids for around 70% of energy generation, the remainder being provided predominantly by glucose. In the early stages of heart failure, the heart relies more heavily on glucose, whereas in the late stages both fatty acid and glucose oxidation are reduced, leading to energetic impairment and reduced systolic function. Glucose oxidation is controlled by the multienzyme complex, pyruvate dehydrogenase (PDH), linking glycolysis in the cytosol with the tricarboxylic acid cycle in the mitochondrial matrix. In this work, we manipulated substrate availability in the rodent heart by three different ways: Depletion of plasma non-esterified fatty acids (NEFA) with the nicotinic acid analogue acipimox, overnight fasting to decrease plasma glucose levels and combined fasting and reduction of NEFA. We assessed plasma substrate levels and subsequently performed multiparametric MRI to assess cardiac function with a CINE FLASH sequence and cardiac metabolism with hyperpolarized [1-13C]pyruvate, with PDH flux as a primary endpoint.Methods
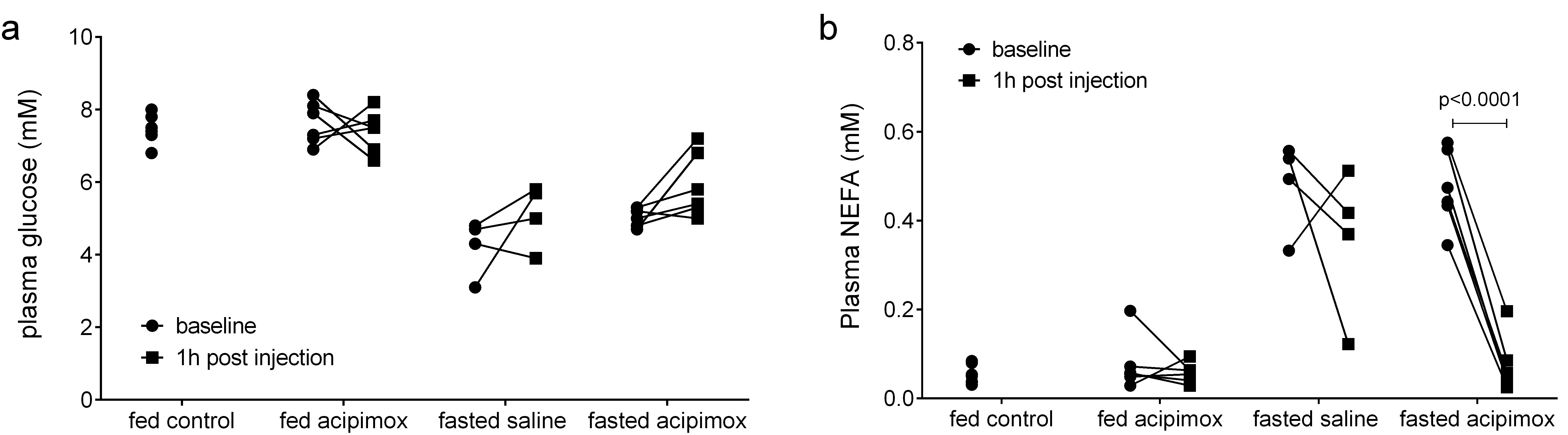
24 weight-matched male Wistar rats were randomized into 4 groups: a fed control group (n=8), a fed group receiving an i.p. injection of 50mg/kg acipimox (n=6) to reduce circulating free fatty acids, an overnight fasted group receiving acipimox (n=6) and an overnight fasted group receiving an i.p. injection of 2mL/kg saline (n=4). Blood samples were taken before the i.p. injection and one hour after the i.p injection for analysis of blood glucose with a glucometer (AccuCheck) and analysis of NEFA with a spectrophotometric assay kit (Randox). Rats then underwent a multiparametric MRI protocol on a 7T horizontal bore spectrometer (Varian) between 1 and 2 hours post i.p. injection. A CINE FLASH sequence was employed to assess cardiac function and hyperpolarized [1-13C]pyruvate MRS was performed to assess cardiac PDH flux2. One mL of 80 mM hyperpolarized [1-13C]pyruvate was injected into the tail vain over 10s. Slice selective 13C MR spectra were acquired from the heart (10 mm slab) every second for 60s using a 72-mm dual-tuned birdcage volume transmit 1H/13C coil and a 13C two-channel surface receive coil (Rapid Biomedical; 15º sinc pulse; 13kHz bandwidth). Multicoil spectra were added in phase and analyzed in AMARES/jMRUI3. CINE images were analyzed with the free-hand drawing function in ImageJ (NIH).Results
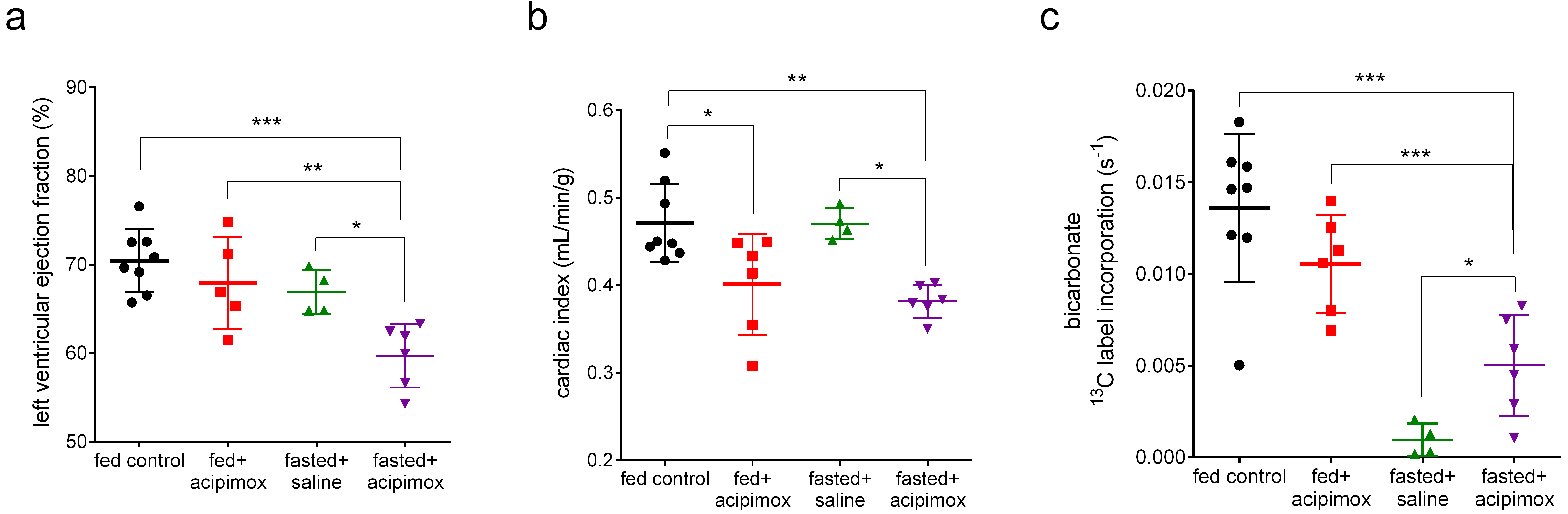
Fed control and fed acipimox treated rats had baseline blood glucose levels of 7.4±0.4 mM and 7.6±0.6 mM respectively. Fasted saline treated and fasted acipimox treated rats had lower baseline blood glucose levels of 4.2±0.8 mM and 5.1±0.3 mM, respectively (Figure 1a). Plasma NEFA levels were lower in fed than in fasted rats (0.05±0.2 mM and 0.08±0.06 mM vs 0.48±0.40 mM and 0.47±0.09 mM, respectively). These NEFA levels did not change after acipimox injection into fed rats or after saline injection into fasted rats but there was a significant decrease in NEFA levels in fasted rats treated with acipimox down to “fed” levels (0.07±0.06 mM, Figure 1b). Cardiac left ventricular ejection fraction was significantly decreased between 1 and 2 hours after acipimox injection in fasted rats but unchanged by any other intervention (Figure 2a). Interestingly, cardiac index was significantly decreased in both fed and fasted rats after acipimox injection (Figure 2b). As expected, PDH flux was decreased in fasted saline treated rats compared to fed control rats (Figure 2c). Acipimox treatment appeared to decrease PDH flux in fed rats, although this was not significant (p=0.06). Acipimox increased PDH flux significantly in fasted rats, however, it did not reach values measured in fed rats.Discussion
Decreasing NEFA levels in fasted rats led to reduced cardiac systolic function. PDH flux was increased, however, this did not reach levels seen in fed rats, which may result in inadequate cardiac energetics leading to reduced systolic function. Acipimox may furthermore have off-target effects directly affecting PDH activity as fed rats treated with acipimox showed decreased cardiac systolic function despite maintained NEFA levels and had an, albeit not significant, reduction in PDH flux.Conclusions and future direction
We have shown that NEFA depletion in the plasma in fasted rats leads to reduced cardiac systolic function and that the mechanism of this fall appears to be insufficient upregulation of PDH flux. This proves the concept that substrate manipulation is related to function, provides a novel model for the energetically starved heart failure state, and provides evidence that PDH flux is a potential therapeutic target for heart failure.Acknowledgements
This work was supported by a British Heart Foundation Immediate Postdoctoral Basic Science Research Fellowship (KNT, FS/16/7/31843), a British Heart Foundation Clinical Research Fellowship (WDW, FS/17/4/832907), a British Heart Foundation Intermediate Clinical Research Fellowship (OJL) and a British Heart Foundation Senior Fellowship (DJT, FS/14/17/30634).References
1. Neubauer S. The failing heart--an engine out of fuel. N Engl J Med. 2007;356(11):1140-1151. doi:10.1056/NEJMra063052.
2. Schroeder MA, Cochlin LE, Heather LC, Clarke K, Radda GK, Tyler DJ. In vivo assessment of pyruvate dehydrogenase flux in the heart using hyperpolarized carbon-13 magnetic resonance. Proc Natl Acad Sci. 2008;105(33):12051-12056. doi:10.1073/pnas.0805953105.
3. Vanhamme L, Van Den Boogaart A, Van Huffel S. Improved Method for Accurate and Efficient Quantification of MRS Data with Use of Prior Knowledge. J Magn Reson. 1997;129(1):35-43. doi:10.1006/jmre.1997.1244.
Figures