2152
The Prognostic Role of Syncope and Cardiac Magnetic Resonance Based Left Ventricular Myocardium Deformation in Arrhythmogenic Right Ventricular Cardiomyopathy(ARVC) Patients1Department of Radiology, West China Hospital, Sichuan University, Chengdu, China, 2MR Collaboration, Siemens Healthcare Ltd., Shanghai, China., Chengdu, China, 3West China Second University Hospital, Sichuan University, Chengdu, China
Synopsis
To explore prognostic role of clinical characteristics and CMR based strains in ARVC patients. CMR was performed in 45 ARVC patients. LV global strains in ARVC patients was significantly reduced than controls. Patients with syncope had statistically lower LV global stains and greater LGE incidence than without syncope. At 1037.51 ± 603.38 days mean follow-up, 14 patients reached end point. By univariate and multivariate regression analysis, syncope (OR= 48.66, [4.20-564.46]; P=0.002) and GLS> -12.72% (OR= 16.96, [1.79-160.66]; P=0.014) remained significantly associated with end point. Therefore, our study found syncope and GLS> -12.72% could predict adverse events in patients with ARVC
Purpose
To explore prognostic role of clinical characteristics and cardiovascular magnetic resonance (CMR) based strain parameters in arrhythmogenic right ventricular cardiomyopathy (ARVC) patients.Methods
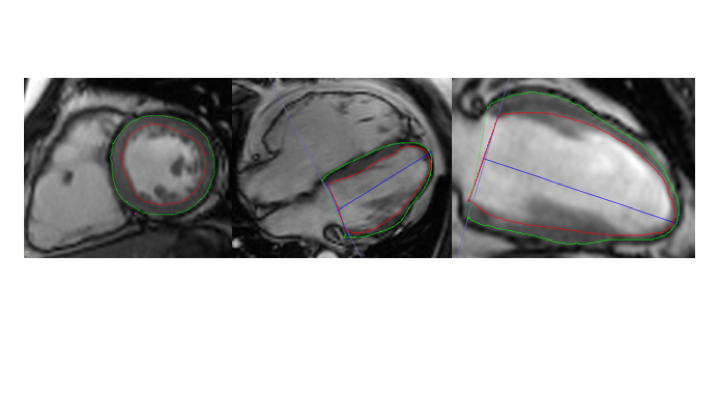
CMR was performed in 45 ARVC patients and 34 healthy controls using a 3T MR scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany). Feature-tracking analysis was applied to cine CMR images on a commercial post-processing image station (Figure 1). Follow-up was performed at least 6-month intervals after CMR scan. The outcome measure was a composite of end points: sudden cardiac death, cardiac arrest, sustained ventricular tachyarrythmias, appropriate implantable cardioverter defibrillator (ICD) shock and heart transplantation. Receiver- operating characteristic (ROC) method was used to determine the optimal cut-off values for the prediction of the endpointsResults
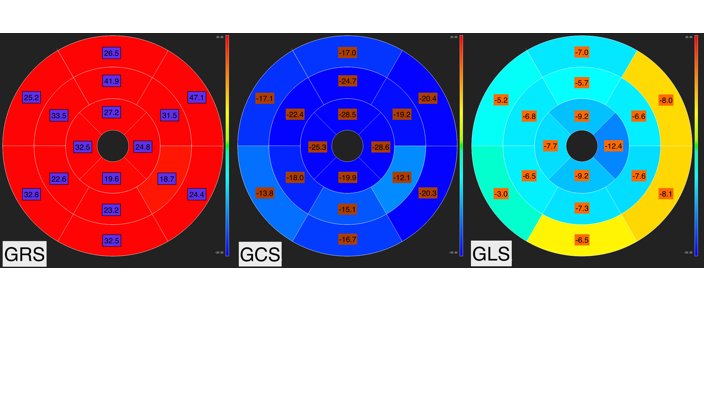
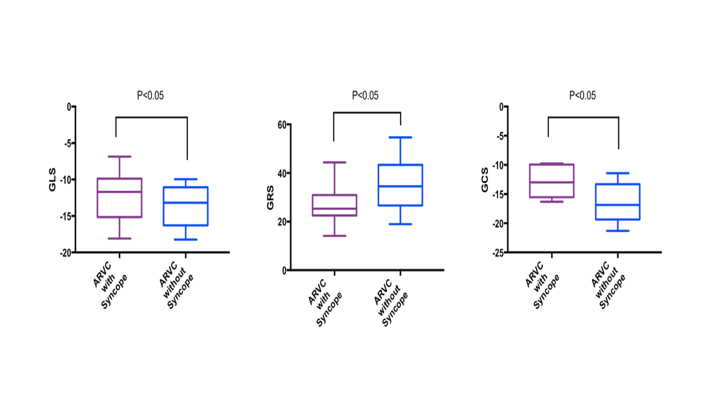
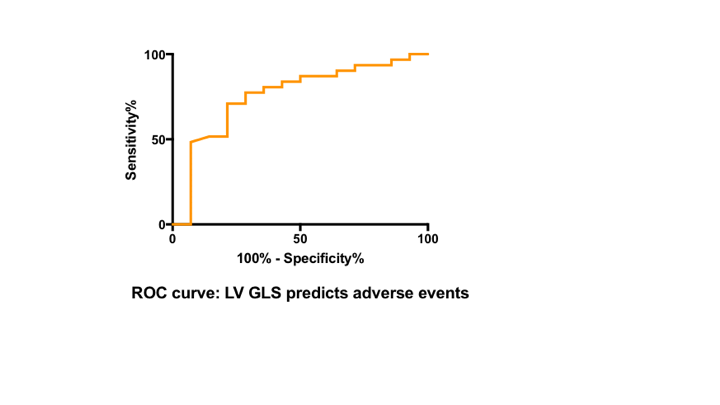
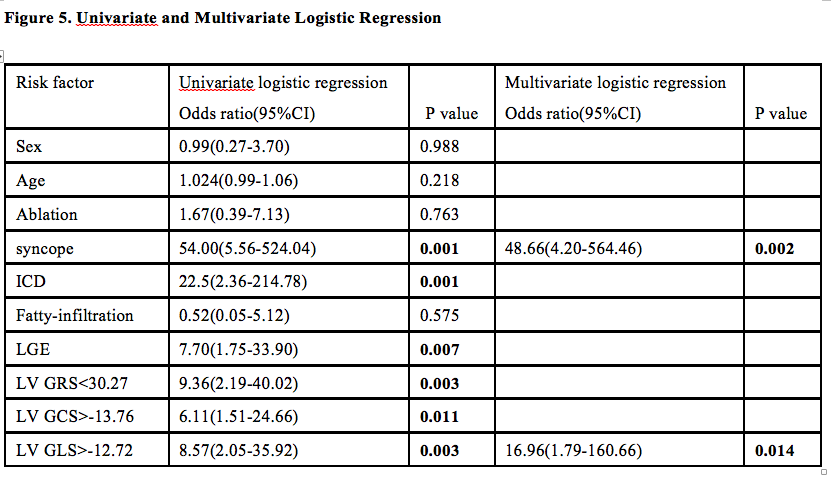
LV GLS (-14.17± 3.29% vs. -16.68 ± 2.74%), GCS (-15.86 ± 3.52% vs. -19.20 ± 2.23%), GRS (35.14 ± 11.97% vs. 49.92 ± 12.59%) in ARVC was significantly reduced in comparison with controls (P<0.001 for all)(Figure 2). Patients with syncope had statistically lower LV GLS (-12.87 ± 3.09% vs. -14.60 ± 3.32%), GCS (-13.87 ± 3.09% vs. -16.34 ± 3.46%), GRS (28.22 ± 7.23% vs. 37.11 ± 23.38%) and greater LGE incidence (70% vs. 40%) than that of patients without syncope (p<0.05 for all)[1] (Figure 3). At 1037.51 ± 603.38 days mean follow-up, 14 patients reached the end point. Patients GLS > -12.72% could predict outcome with a sensitivity of 77.42% and specificity of 71.43%(AUC=0.759, p< 0.05)(Figure 4). By univariate analysis, several clinical and CMR parameters including history of syncope, ICD, presence of LGE and LV GLS> -12.72% were predictors of the endpoint. However, multivariable analysis for the end point revealed only syncope (OR= 48.66, [4.20-564.46]; P=0.002) and GLS> -12.72% (OR= 16.96, [1.79-160.66]; P=0.014) as independent predictors.(Figure 5)Discussion and Conclusions
CMR-based Global strains of the left ventricle have shown to be reduced in ARVC patients[2], which is less operator-dependent than visual wall motion analysis. After following up 45 patients with ARVC for a median of 1037.51 days, we found syncope and GLS> -12.72% could predict adverse events in patients with ARVC and may help to optimize risk stratification in these patients[3]. Further, properly designed prospective studies are warranted to confirm these findings.Acknowledgements
This work was supported by the National Natural Science Foundation of China (81471721, 81471722, 81571668, 81771887, and 81771897)References
[1]: Cheng H, Lu M, Hou C, et. al Comparative study of CMR characteristics between arrhythmogenic right ventricular cardiomyopathy patients with/without syncope. Int J Cardiovasc Imaging. 2014 Oct;30(7):1365-72
[2]: Heermann P, Hedderich DM, Paul M, et.al. Biventricular myocardial strain analysis in patients with arrhythmogenic right ventricular cardiomyopathy (ARVC) using cardiovascular magnetic resonance feature tracking. J Cardiovasc Magn Reson. 2014 Oct 7;16:75
[3]: 2018 ESC Guidelines for the diagnosis and management of syncope. Rev Esp Cardiol (Engl Ed). 2018 Oct;71(10):837
Figures