2150
Doxorubicin induced cardiotoxicity highlighted from the combination of CMR, exercise tests data and CircAdapt model.1Polytechnique Montreal, Montreal, QC, Canada, 2Université de Montréal, Montreal, QC, Canada
Synopsis
This study aims to discriminate three risk groups of leukemia survivors investigating subtle changes in their myocardium mechanical properties. Volumes extracted from cine-MRI images coupled to incremental exercise data allowed the quantification of the mechanical properties of the left ventricle using a reverse material identification approach based on the CircAdapt model. While both passive and active properties did not show significant changes in ALL survivors between risk groups, the increased arteriovenous pressure drop suggested that the cardioprotective agent entailed a compensation of the cardiac function through the peripheral components of the oxygen delivery chain.
Introduction
Acute Lymphoblastic Leukemia (ALL) is currently treated using doxorubicin-based chemotherapy, which effectiveness has been proven [1]. However, it induces a wide spectrum of dose-dependent cardiotoxicity [2] affecting the myocardium at both morphological and functional levels. The mechanical properties of the myocardium could be adequate indicators of the tissue’s viability. Reverse identification methods based on MRI, intraventricular pressure measurements and finite element models were proposed but the pressure measured by catheter cannot be considered in children. The parameterized numerical model CircAdapt, which enables live simulation of the interaction between the different walls of the myocardium [3], can be associated to exercise tests to personalize tissue’s properties. The objective of this study was to characterize subtle changes in the mechanical properties of the left ventricle in a cohort of childhood ALL survivors according to their prognostic risk using the CircAdapt model combined to exercise tests data and cine-MRI images.Methods
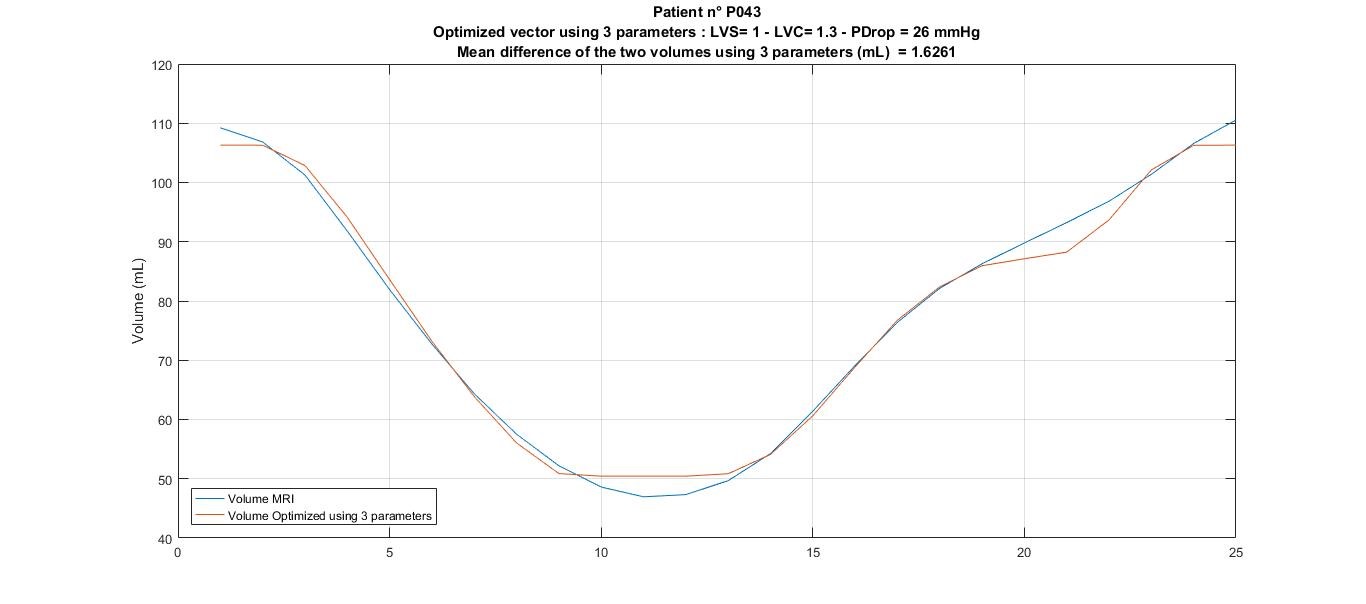
Forty-seven ALL survivors (23±6 years old) were prospectively included and divided into 3 groups according to their exposition risk to doxorubicin: standard risk (SR, n=14), high risk (HR, n=17) and high-risk group who received dexrazoxane, a cardioprotective agent (HRdex, n=16). They all experienced an incremental exercise test (cycle ergometer, Oxycon Pro, Jaeger) coupled with cardiac hemodynamic monitoring (PhysioFlow, Manatec Biomedical). The four basic inputs of the CircAdapt model were evaluated: heart rate (HR), cardiac output (CO), diastolic arterial pressure (DAP) and systolic arterial pressure (SAP). All the ALL survivors underwent a CMR acquisition including an ECG-gated cine TruFISP sequence at 3T (Siemens SkyraTM) using an 18-channel phased array body matrix coil. For each slice (14 slices in short axis and 4 slices in long axis), 25 phases of the cardiac cycle were acquired during multiple breath-holds. The endocardial volume of the left ventricle was quantified from a semi-automatic segmentation (CIM v8.1, University of Auckland). A sensitivity analysis of the CircAdapt model was performed using the Morris method (r=36 trajectories, p=10 levels and n=23 inputs [4, 5]) to identify the most influencing parameters. These parameters were then included in an optimization problem to personalize the cardiac mechanical properties from the minimization of the difference between the MRI volumes and the CircAdapt estimated volumes (Figure 1). A one-way ANOVA was performed on the optimized parameters to compare the risk groups.Results
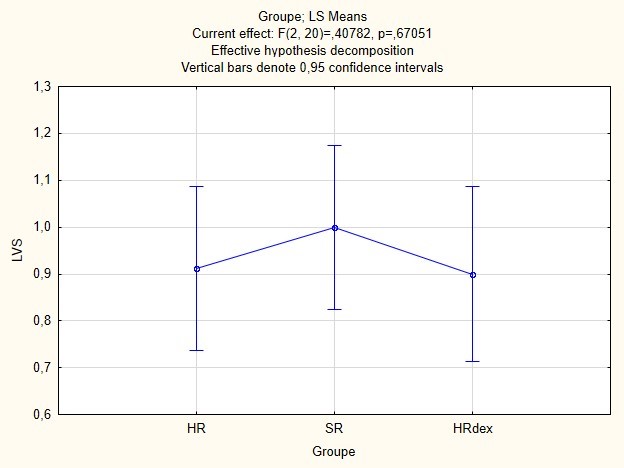
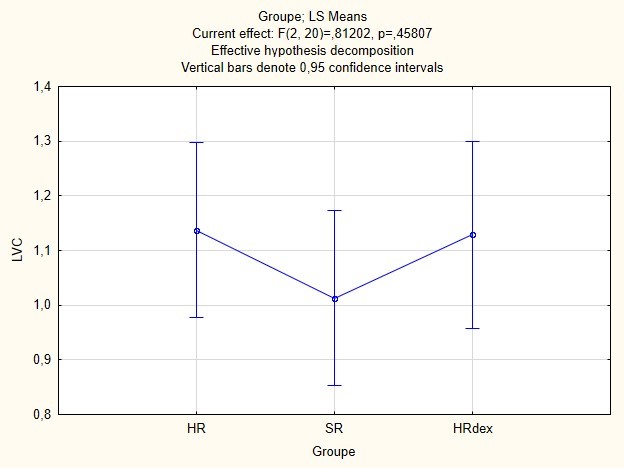
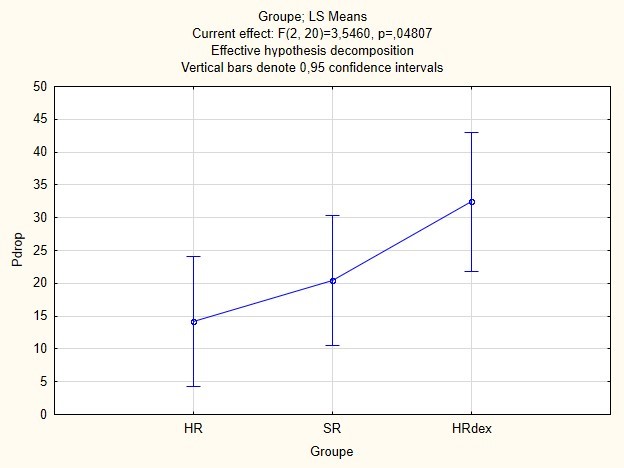
The sensitivity study of the CircAdapt model showed that the left ventricle stiffness (LVS), the left ventricle contractility (LVC) and the arteriovenous pressure drop (Pdrop) were the most influencing parameters. No significant differences were observed on LVS and LVC between the three groups (p>0.05, Figures 2 and 3). However, LVS tends to be smaller (-10%) while LVC tends to be higher (+10%) in both HR and HRdex groups as compared to SR and “CircAdapt” healthy groups. Significant differences were observed on Pdrop between the three groups (p=.048, Figure 4). The HR group appears to be the closest to the nominal values of 11 mmHg of CircAdapt while increasing for SR and HRdex groups.Discussion
Both passive and active mechanical properties of the left ventricle of the SR group, who received the lowest dose of anthracycline, were expected to be similar to the ones of healthy volunteers. However, the subtle changes found in the HR group were not expected to be also found in the HRdex groups who received a cardioprotective agent, suggesting a lack of effectiveness of the dexrazoxane on the mechanical properties of the left ventricle. The large increase of the arteriovenous pressure drop in the HRdex group (three time the nominal value) suggested a compensation of the functional condition of the heart by the central nervous system through the peripheral components of the oxygen delivery chain. Among the 47 patients, only 23 of them showed reliable optimization results (mean volume differences less than 11ml that is the mean difference obtained for the 47 survivors), decreasing the power of the statistical tests. The CircAdapt model showed limitations in representing an early systole peak that appears around the 7th frame (instead of 11th) over 25 frames.Conclusion
Volumes extracted from cine-MRI images coupled to incremental exercise data allowed the quantification of the mechanical properties of the left ventricle using a reverse material identification approach based on the CircAdapt model. While both passive and active properties did not show significant changes in ALL survivors between risk groups, the increased arteriovenous pressure drop suggested that the cardioprotective agent entailed a compensation of the cardiac function through the peripheral components of the oxygen delivery chain.Acknowledgements
NSERC, Polytechnique Montreal and the Foundation Arbour for the financial support, researchers from the PETALE study for the opportunity to do this complementary analyses on the cancer survivors.References
1. Singal, P.K. and N. Iliskovic, Doxorubicin-Induced Cardiomyopathy. New England Journal of Medicine, 1998. 339(13): p. 900-905.
2. Chatterjee, K., et al., Doxorubicin cardiomyopathy. Cardiology, 2010. 115(2): p. 155-62.
3. Arts, T., et al., Adaptation to mechanical load determines shape and properties of heart and circulation: the CircAdapt model. Am J Physiol Heart Circ Physiol, 2005. 288(4): p. H1943-54.
4. Morris, M.D., Factorial Sampling Plans for Preliminary Computational Experiments. Technometrics, 1991. 33(2): p. 161-174.
5. Campolongo, F., J. Cariboni, and A. Saltelli, An effective screening design for sensitivity analysis of large models. Environmental Modelling & Software, 2007. 22(10): p. 1509-1518.
Figures