2149
Self-Navigated, Free-Breathing 3D Left Atrial Late Gadolinium Enhancement MRI with Stack-of-Stars k-space Sampling and GRASP Reconstruction: A Preliminary Study for Quantification of Atrial Fibrosis1Northwestern University, Chicago, IL, United States
Synopsis
Given the thin nature of the left atrial (LA) wall (1-3 mm) and the need to perform respiratory gating with navigator echoes, the clinical translation of LA late gadolinium-enhanced (LGE) MRI has proven difficult. This study describes a self-navigated, free-breathing 3D LA LGE pulse sequence with stack-of-stars k-space sampling and GRASP reconstruction. This study shows initial experience in quantifying LA fibrosis in patients with atrial fibrillation undergoing ablation therapy.
Introduction
Left atrial (LA) fibrosis is considered a substrate responsible for the initiation and maintenance of atrial fibrillation (AF)1,2. LA fibrosis as measured by late gadolinium enhancement (LGE) MRI3 has been shown to predict AF recurrence following AF ablation4. Unfortunately, due to the thin nature of the LA wall (1-3 mm)5 and the need to perform respiratory gating with navigator echoes, the clinical translation of LA LGE MRI has proven difficult. One approach to improve the reproducibility of LA LGE is by performing self-navigated, free-breathing imaging. The purpose of this study was to develop a free-breathing 3D LA LGE pulse sequence with stack-of-stars k-space sampling and GRASP reconstruction6 and quantify LA fibrosis in AF patients undergoing AF ablation.Methods
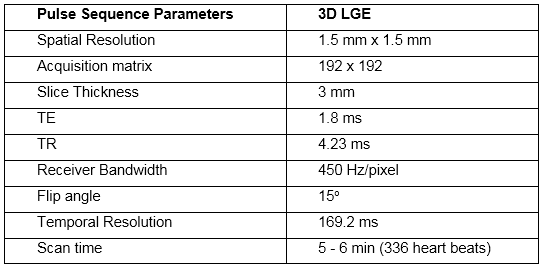
Human Subjects & Pulse Sequence: Eight AF patients (5 males, mean age = 59 ± 10 years) scheduled for AF ablation were scanned on a 1.5 T scanner (Siemens, AERA or AVANTO). We modified a previously described 3D stack-of-stars GRASP reconstruction method7 for performing 3D LA LGE. The relevant imaging parameters are summarized in Table 1. 3D LA LGE was performed in a 2 chamber view sampling the left side of the heart, approximately 5-10 minutes after administration of 0.15 to 0.20 mmol/kg of gadobutrol (Gadavist, Bayer). Imaging was performed under free breathing over 336 heart beats (or 5-6 minutes).
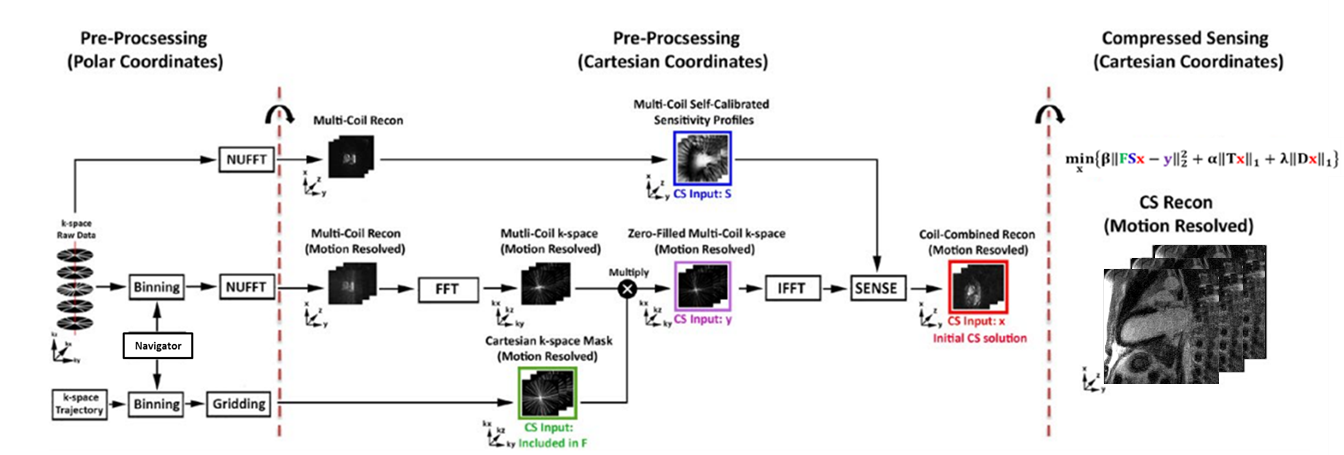
Image Reconstruction: The GRASP reconstruction was performed off-line as previously described7, except for this study we used both temporal total variation and temporal principal components as two orthogonal sparsifying transforms (Figure 1). Regularization weights were determined empirically based on visual analysis of training data sets. Self-calibration of respiratory motion was used to bin the data into 6 respiratory states, as previously described7, and the respiratory frame with the best image quality was visually selected for analysis. After reconstruction, the image was interpolated in the slice direction such that slice thickness for analysis was 1.5 mm. We additionally applied block matching to further suppress noise8 and surface coil correction using previously described method9.
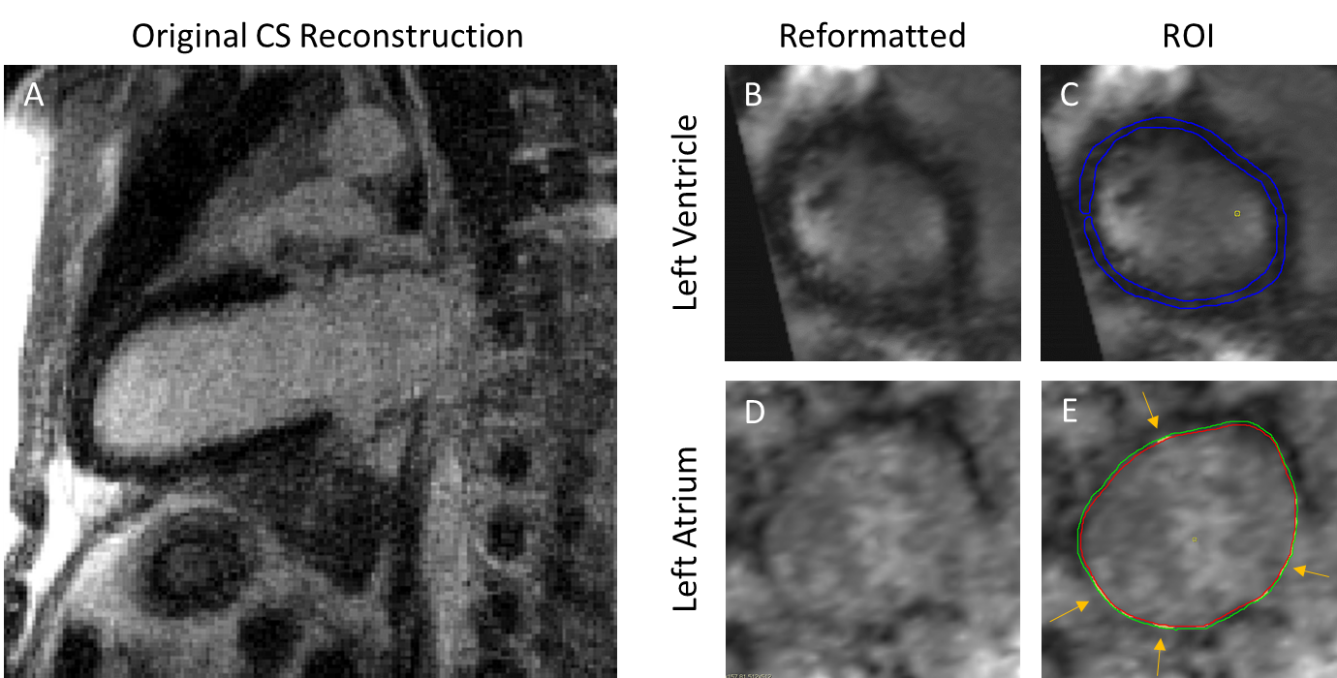
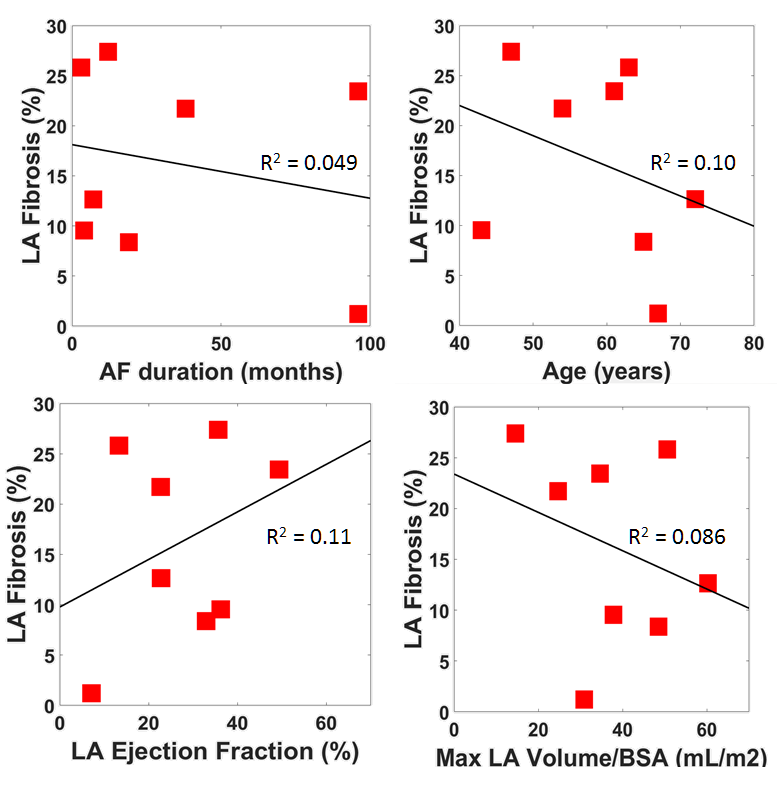
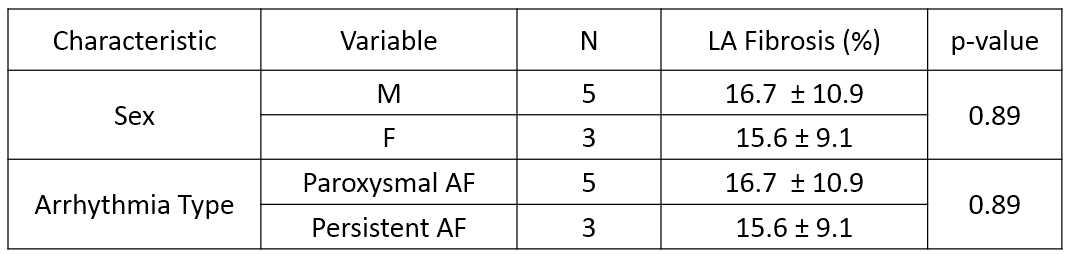
Data Analysis: For LA fibrosis measurements, the 2 chamber view was reformatted in CVI42 (Circle Cardiovascular Imaging Inc.) to a short axis stack view. Reference myocardium ROIs were drawn in the left ventricle (LV) myocardium. In the LA, endocardial and epicardial contours were manually drawn at the LA border. Fibrosis was determined to be signal > 6x standard deviation of the reference (Figure 2). LA volumes were calculated by the area-length method10 and body surface area (BSA) as determined by the Mosteller formula. LA fibrosis was compared to AF duration, age, LA ejection fraction, and maximum LA volume/BSA using linear regression. Furthermore, Two-tailed t-tests assuming equal variance were used to compare LA fibrosis to sex and AF type.
Results
Accelerated 3D LA LGE produced good image quality after CS reconstruction and denoising (Figure 2A). In our patient cohort, mean LA fibrosis was 16.3 ± 9.6%. We did not detect any correlation of LA fibrosis to AF duration, age, LA ejection fraction, or maximum LA volume/BSA (Figure 3). Additionally, no significant difference was shown between sex or AF type in LA fibrosis (Table 2).Discussion
The proposed 3D LA LGE MRI method with stack-of-stars k-space sampling and GRASP reconstruction produced good image quality and LA fibrosis levels that are consistent with a prior study4. Possible sources of error include using myocardium that is not sufficiently nulled for the reference. Additionally, manually drawing LA contours was challenging due to suboptimal spatial resolution and/or contrast to noise ratio. A future study is warranted to enroll more patients and determine any LA fibrosis trends that could result in improvement to clinical outcomes.Acknowledgements
This work was supported in part by the following grants: NIH R01HL116895, R01HL138578, R21EB024315, R21AG055954References
1. Dzeshka MS, Lip GY, Snezhitskiy V, Shantsila E. Cardiac Fibrosis in Patients With Atrial Fibrillation: Mechanisms and Clinical Implications. J Am Coll Cardiol 2015;66:943-59.
2. Goldberger JJ, Arora R, Green D et al. Evaluating the Atrial Myopathy Underlying Atrial Fibrillation: Identifying the Arrhythmogenic and Thrombogenic Substrate. Circulation 2015;132:278-91.
3. Peters DC, Wylie JV, Hauser TH et al. Detection of pulmonary vein and left atrial scar after catheter ablation with three-dimensional navigator-gated delayed enhancement MR imaging: initial experience. Radiology 2007;243:690-5.
4. Akoum N, Daccarett M, McGann C et al. Atrial fibrosis helps select the appropriate patient and strategy in catheter ablation of atrial fibrillation: a DE-MRI guided approach. Journal of cardiovascular electrophysiology 2011;22:16-22.
5. Tan HW, Wang XH, Shi HF, Zhou L, Gu JN, Liu X. Left atrial wall thickness: anatomic aspects relevant to catheter ablation of atrial fibrillation. Chin Med J (Engl) 2012;125:12-5.
6. Feng L, Grimm R, Block KT et al. Golden‐angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden‐angle radial sampling for fast and flexible dynamic volumetric MRI. Magnetic resonance in medicine 2014;72:707-717.
7. Haji-Valizadeh H, Collins JD, Aouad PJ et al. Accelerated, free-breathing, noncontrast, electrocardiograph-triggered, thoracic MR angiography with stack-of-stars k-space sampling and GRASP reconstruction. Magn Reson Med 2018.
8. Dabov K, Foi A, Katkovnik V, Egiazarian K. Image denoising by sparse 3-D transform-domain collaborative filtering. IEEE transactions on image processing : a publication of the IEEE Signal Processing Society 2007;16:2080-95.
9. Ren H, Lin W, Ding X. Surface Coil Intensity Correction in Magnetic Resonance Imaging in Spinal Metastases. Open Med (Wars) 2017;12:138-143.
10. Jiamsripong P, Honda T, Reuss CS et al. Three methods for evaluation of left atrial volume. Eur J Echocardiogr 2008;9:351-5.
Figures