2142
Manifold recovery in cardiac dynamic MRI (dMRI) with different reduction factors1Center for Biomedical Imaging Research, Department of Biomedical Engineering, School of Medicine, Tsinghua University, Beijing, China, 2Electrical Engineering, University at Buffalo, State University of New York, Buffalo, NY, United States, 3Biomedical Engineering, University at Buffalo, State University of New York, Buffalo, NY, United States, 4Department of Radiology, University of Washington, Seattle, WA, United States
Synopsis
Manifold models have been developed as an effective tool in dynamic MRI recently. With the abilities of characterizing the relationship between dMRI images series, they could be used to reconstruct high-quality image series from MRI data sampled below the Nyquist rate. However, the amount of MRI data required by manifold recovery is not clear yet. In this study, we did some simulation experiments to investigate the relationship between image quality of cardiac dynamic MRI and reduction factor, and proposed an optimized reduction factor considering both image quality and acquisition efficiency.
Introduction
Conventional dMRI requires models based on algorithms such as parallel imaging, compressed sensing or sparsity and low-rank constraints1 to reconstruct sub-Nyquist sampling data, which always need very long reconstruction time to get high temporal resolution image series. While, manifold method2 can solve the problem, it can shorten the reconstruction time and maintain high temporal resolution simultaneously due to its lower computational complexity. However, the minimum amount of acquisition data required by manifold recovery has not been investigated. In this study, we did some simulation experiments to evaluate the image quality with different reduction factors for manifold recovery in cardiac dynamic MRI and tried to propose an optimized reduction factor.Methods
Data source: The data was collected on a 3.0 T whole-body MR scanner (Achieva, Philips Medical System, Best, The Netherlands) with a 32-channel cardiovascular coil using a balanced fast field echo (FFE) pulse sequence. The scan region involved all left atrium and left ventricle. The scan parameters were: FOV = 247mm×247mm(RL/AP), voxel size = 1.8mm×1.4mm(RL/AP), data matrix size = 168×272×30, TR/TE = 2.9ms/1.45ms, temporal resolution = 32.5ms, flip angle = 40°. The undersampling pattern was the same as reference2. Reconstruction: Different reduction factors were used for reconstruction based on the manifold method2 to get the relationship between reduction factor and image quality. Comparison: The structural similarity (SSIM)3 and signal-to-noise ratio(SNR) were calculated on results to evaluate the performance. Specifically, we compared the SSIM and SNR on three time frames corresponding to the end of systole, the mid-diastole and the end of diastole respectively. SSIM of each frame was calculated between each reconstruction result and corresponding full k-space reconstruction result. SNR of each frame was obtained by dividing the standard deviation of the signal portion by the standard deviation of the background noise portion in each reconstruction result.Results
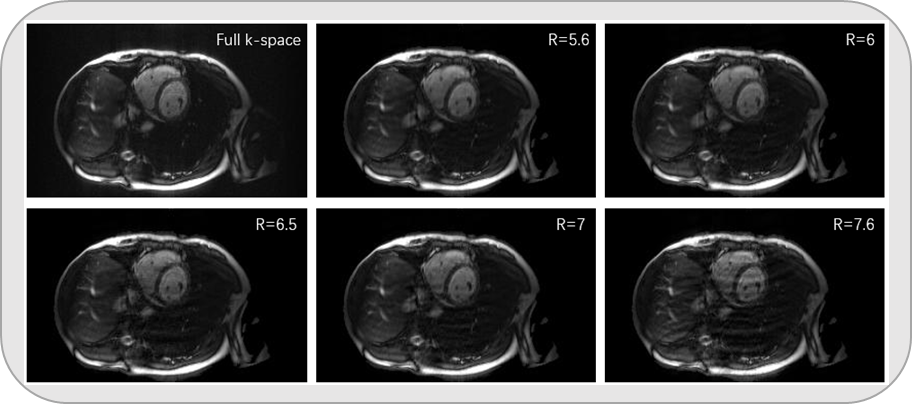
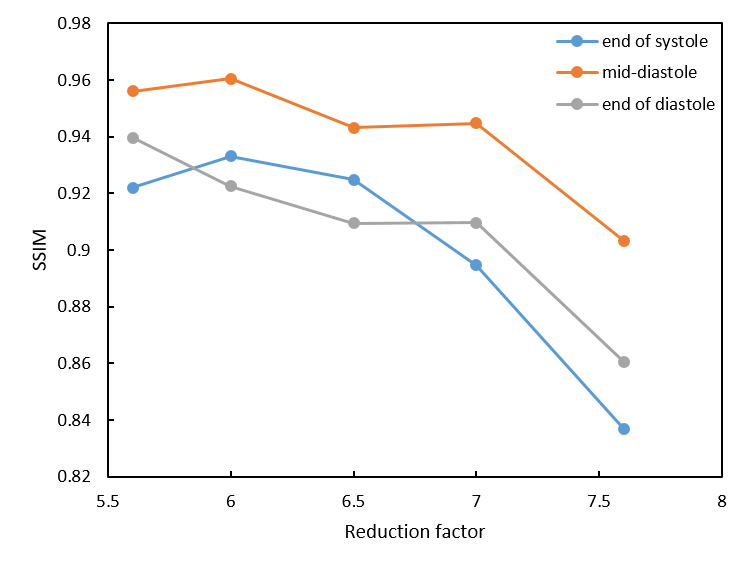
Reconstructed magnitude maps (in the end of systole) at different reduction factors were shown in Figure 1. We can see that when reduction factor smaller than 7, the reconstructed images showed good agreements with fully sampled reference within region-of-interest. While when reduction factor larger than 7, there appeared a lot of artifacts in the reconstructed image. Figure 2 showed the SSIM curves with the increase of reduction factor. The overall trends of the curves were decreasing. When reduction factor > 7, SSIM decreased rapidly. Specifically, the mid-diastole curve performed best, which is because the end of systole and the end of diastole changed sharply, resulting in relatively poor reconstruction results along the temporal direction. Figure 3 showed the SNR curves. Similar to the magnitude maps and SNR curves, with the growth of reduction factor, SNR declined rapidly when reduction factor > 7.Discussion
We investigated the relationship between reduction factor and image quality for manifold recovery in cardiac dynamic MRI in this study. With the increase of reduction factor, the image quality declined and became unacceptable due to the large number of artifacts when reduction factor > 7. The point of reduction factor = 7 was a turning point of SSIM and SNR curves. So, the reduction factor = 7 was the optimized reduction factor for manifold recovery of cardiac dynamic imaging. Future study can be performed to try to combine the manifold models with parallel imaging, compressed sensing or sparsity constraints models to raise the temporal resolution of dynamic MRI without the significant extension of reconstruction time.Conclusion
In this study, we used the manifold method2 to reconstruct the cardiac dynamic imaging from different reduction factors, and assessed the image quality with different amount of data associated with different reduction factors, which can provide an optimized reduction factor for manifold recovery in cardiac dynamic MRI.Acknowledgements
No acknowledgement found.References
[1] Tsao J, Kozerke S. MRI temporal acceleration techniques[J]. Journal of Magnetic Resonance Imaging, 2012, 36(3): 543-560.
[2] Nakarmi U, Wang Y, Lyu J, et al. A kernel-based low-rank (klr) model for low-dimensional manifold recovery in highly accelerated dynamic mri[J]. IEEE transactions on medical imaging, 2017, 36(11): 2297-2307.
[3] Hore A, Ziou D. Image quality metrics: PSNR vs. SSIM[C]//Pattern recognition (icpr), 2010 20th international conference on. IEEE, 2010: 2366-2369.
Figures