2141
Highly accelerated cardiac imaging using a high-density 72 channel local receiver array at 3 Tesla1Department of Radiology, University Medical Center Utrecht, Utrecht, Netherlands, 2Biomedical Engineering and Physics, Academic Medical Center, Amsterdam, Netherlands, 3Department of Radiology, Leiden University Medical Center, Leiden, Netherlands, 4Biomedical Engineering and Physics, Amsterdam UMC, University of Amsterdam, Amsterdam, Netherlands, 5MR Coils B.V., Zaltbommel, Netherlands
Synopsis
Cardiac Magnetic Resonance Imaging (CMR) protocols can be extremely time consuming, expensive, and uncomfortable for the patient. The purpose of this study is to evaluated the acceleration performance for CINE CMR in-vivo scans using a 72 channel high-density coil array at 3 Tesla. We demonstrate highly accelerated CINE imaging within a single breath hold with acceptable SNR and minimal SENSE artifacts.
Introduction
There is an urgent need for highly accelerated cardiac imaging to facilitate shorter examination times and increased patient comfort (1). Current clinical examinations can be lengthy because of the need for many patient breath-holds to eliminate breathing motion. A commonly used method for accelerating image acquisition, and thus reducing the breath-hold time and number of breath-holds is parallel imaging (2). However, the gain in speed by parallel imaging (PI) is limited by the signal-to-noise ratio (SNR), which decreases proportional to the coil geometry factor (g-factor) and the square root of the acceleration factor R. Previously we and others have shown with simulations that a large number of small surface coil elements can increase the maximal obtainable acceleration factor, by maximizing SNR and minimizing the g-factor (3-7). Furthermore, with high enough artefact free acceleration, it is possible to migrate from 2D to 3D acquisitions, thereby overcoming the limitations of low SNR. The purpose of this study is to investigate the maximal obtainable acceleration performance for in-vivo scans using a custom-built high-density 72 channel receive coil.Methods
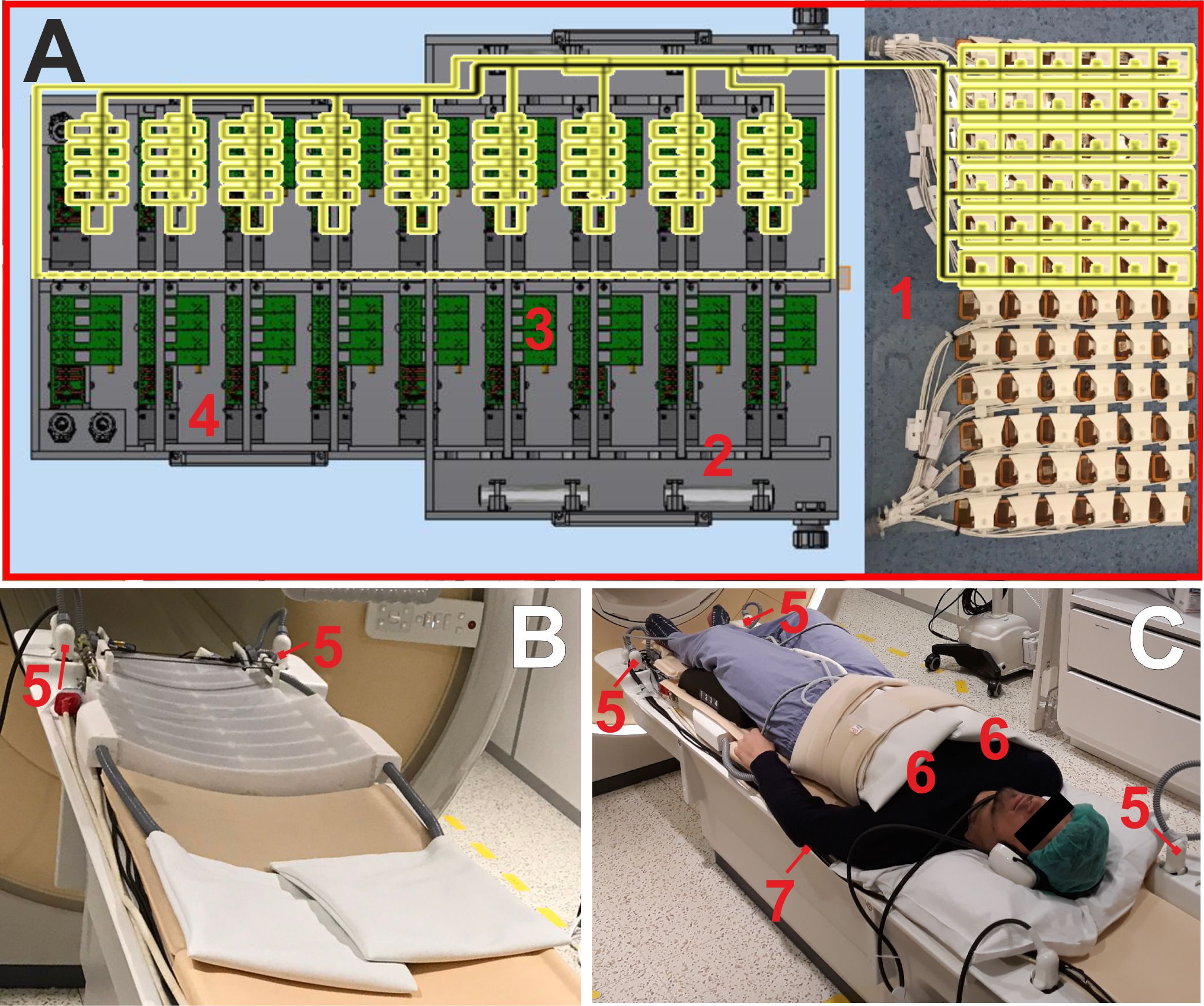
A dedicated high-density 72-channel cardiac array (MRCoils, Zaltbommel, Netherlands) combined with a 12-channel posterior coil in the patient table were used (Fig. 1) resulting in 84 receive channels. Measurements were performed on a Philips 3T Ingenia system with dStream architecture (Philips, Best, Netherlands). The high-density interface box contains the pre-amplifiers which are placed directly on top of the digital receivers. All 72-receiver elements are connected to the pre-amplifiers via cable traps and pre-amplifier decoupling circuits (Fig. 1A). First, to evaluate the accelerating performance, a standard 2D B-SSFP CINE protocol was used (TE = 1.5ms, TR = 3.0ms, FOV 270x270mm, voxel size = 2x2x12mm, FA = 45 degrees, frames = 40). Both short axis and 4 chamber acquisitions were obtained with 2-7 SENSE acceleration. Secondly, a 3D B-SSFP CINE sequence was used to accelerate in two directions (AP-FH, 6 (3x2), 9 (3x3), 12 (4x3), 15 (5x3), 20 (5x4), 25 (5x5); TE = 1.98ms, TR = 4.8ms, FOV 350x350mm, 28 slices, voxel size = 2x2x5mm, FA = 50 degrees, frames = 20). For all scans we used the default Philips reference scans and reconstruction.Results
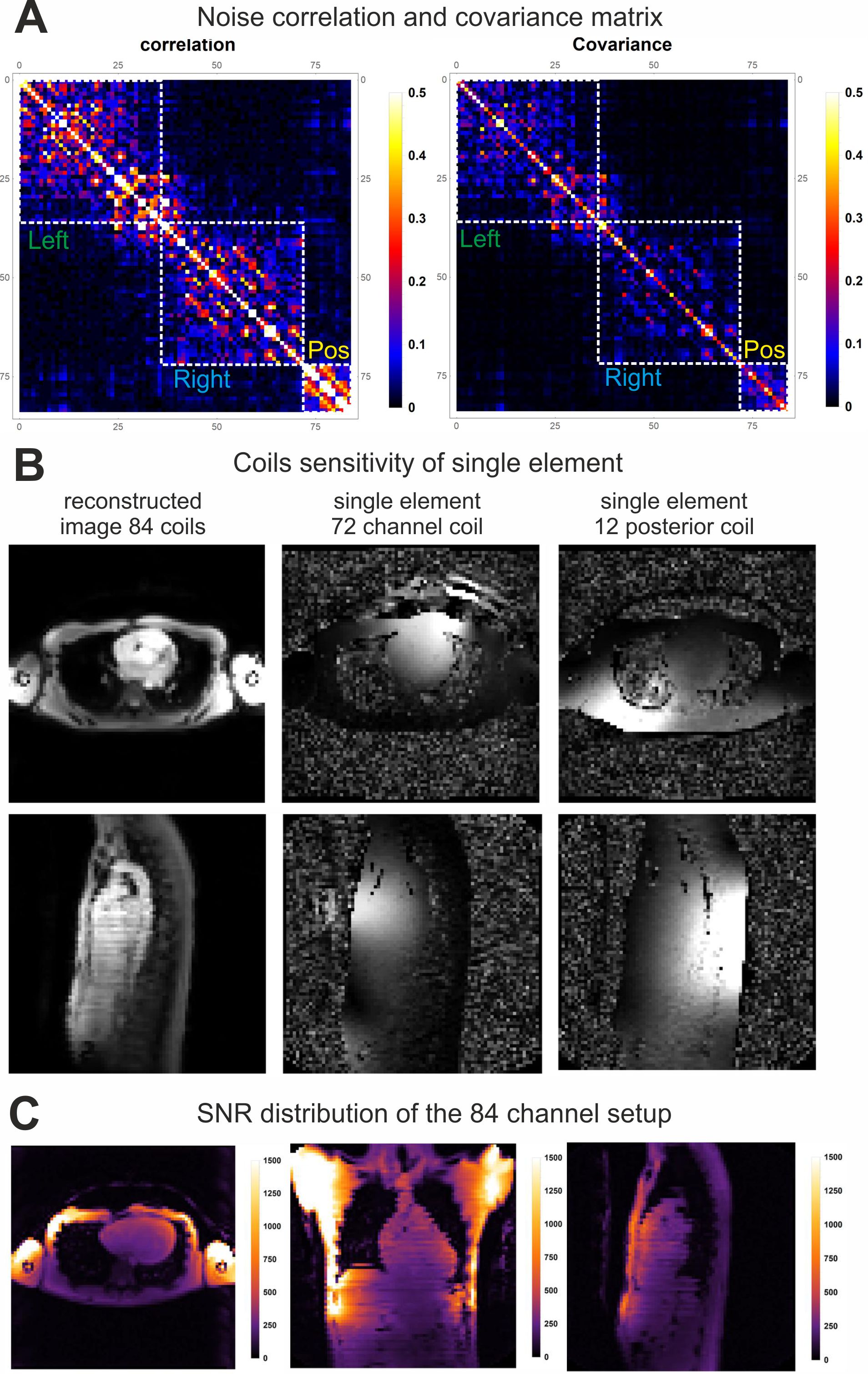
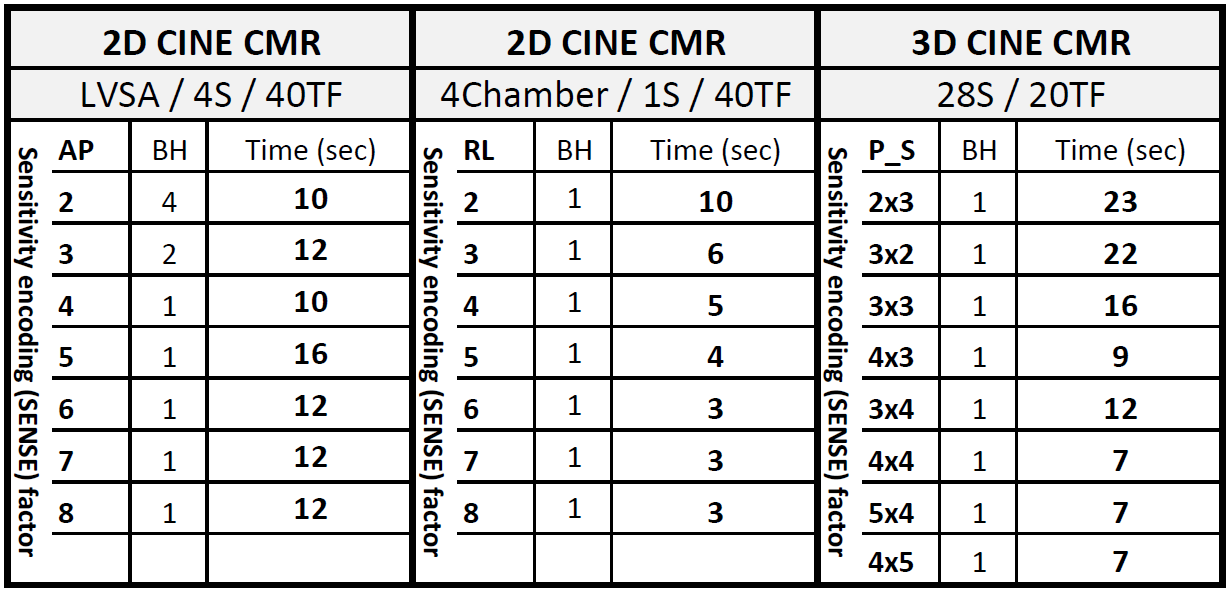
Fig. 2 shows the noise correlation and covariance matrix of the 84-channel coil setup. Additionally, it shows the coils sensitivity and SNR distribution of the setup. Although the coil loops are small their sensitivity is enough to fully cover the torso. Table 1 shows the decreased expiration breath hold time and number of breath-holds while increasing the acceleration factor, using a standard CINE CMR protocol. As expected with increasing SENSE factor the SNR decreases. However, there are no aliasing artifact visible up to 7-fold acceleration (Fig. 3). 3D CINE images acceleration performance shows a 12-fold factor with minimal SNR-drop and a coverage of 28 slices within a single breath-hold expiration of 9 seconds (Fig. 4).Discussion
The results show that in 2D SENSE 7 is feasible without sense artifact but with decreased SNR. In 3D an acceleration factors up to 12 can be obtained with acceptable SNR and limited SENSE artifacts. Performing high accelerated CINE CMR can reduce acquisition time of a single slice to 5 seconds. This will enable potential free breathing scans using respiratory gating. Our 3D acquisition was not optimized and other state of the art 3D acquisitions need to be explored to exclude residual artifacts.Even without the use of compressed SENSE and increasing the number of elements in the posterior array whole heart single BH scans are feasible.Conclusion
We demonstrated high accelerated CINE images in 2D and 3D can be obtained using a high-density coil array. We demonstrated up to 7 times acceleration in 2D, with substantial loss in SNR, but without noticeable SENSE artifacts. With 3D acquisition a 12x acceleration was feasible with limited SENSE artifacts. These results together with previous simulation motivate to further increase the number of receive elements.Acknowledgements
No acknowledgement found.References
(1) M. Saeed, T. A. Van, R. Krug, S. W. Hetts and M. W. Wilson, "Cardiac MR imaging: current status and future direction," Cardiovascular Diagnosis & Therapy, vol. 5, no. 4, pp. 290-310, Aug 2015.
(2) K. P. Pruessmann, M. Weiger, M. B. Scheidegger and P. Boesiger, "SENSE: sensitivity encoding for fast MRI," Magn. Reson. Med., pp. 952-962, 1999.
(3) M. Schuppert, K. F. Kreitner, S. Fischer, S. Wein, B. Keil, L. L. Wald and L. M. Schreiber, "Determination of the optimal number of coil elements: a semi-theoretical approach," in ISMRM, 2015.
(4) R. Etzel, L. Golestanirad, C. Mekkaoui, T. G. Reese, D. E. Sosnovik, A. H. Mahnken and B. Keil, "Receive Coil Array considerations for simultaneous Multislice Imaging in Cardiac MRI," in ISMRM, 2017.
(5) M. Schmitt, A. Potthast, D. E. Sosnovik, J. R. Polimeni, G. C. Wiggins, C. Triantafyllou and L. L. Wald., "A 128-Channel Receive-Only cardiac coil for highly accelerated Cardiac MRI at 3 Tesla," Magn. Reson. Med., vol. 6, pp. 1431-1439, Jun 2008.
(6) C. J. Hardy, R. O. Giaquinto, J. E. Piel, K. W. Rohling, L. Marinelli, D. J. Blezek, E. W. Fiveland, R. D. Darrow and T. K. Foo, "128-channel body MRI with a flexible high-density receiver-coil array," J. Magn. Reson. Imag., vol. 5, pp. 1219-25, Nov 2008.
(7) B.
Gruber, A.J. Hendriks, C. Alborahal, G.J. Strijkers, Gustav, D. Klomp, T.
Leiner, M. Froeling, “A 256-channel Cardiac Coil for accelerated Cardiac
Imaging at 3 Tesla - Evaluation of a 32-channel Prototype” ISMRM 26th
Scientific Meeting & Exhibition, June 2018, Paris, France.
Figures