2138
Evaluation of Cumulative Perimetric Ratio as Quantitative Index for Degree of Left Ventricular Myocardial Trabeculations in Adolescents and Young Adults: Potential Biomarker for Left Ventricular Non-compaction1Texas Children's Hospital, Houston, TX, United States
Synopsis
Balanced steady-state free precession imaging distinguishes the non-compacted left ventricular (LV) myocardial trabeculation (NC) from compacted myocardium (C). However, current diagnostic criterion (NC/C length ratio > 2.3) for left ventricular non-compaction (LVNC) suffers from subjective variability and tends to over-diagnose. Cumulative perimetric ratio (CPR) derived from epi and endocardial contours routinely drawn for LV functional analysis provides comprehensive measure of irregularity and extent of the LV trabeculations overcoming the inherent morphologic variability from base to apex. CPR has a potential to serve as a valuable biomarker for prominent trabeculations, complementary to NC/C length and mass ratios.
PURPOSE
The purpose of this study is to evaluate two-dimensional geometric marker viz. cumulative perimetric ratio (CPR) to quantitate irregularity and extent of the left ventricular (LV) myocardial trabecular structures in bright blood cine balanced steady-state free precession MR images in a pediatric cohort. CPR index can be derived from epi and endocardial contours typically drawn for LV functional analysis, complementary to the morphometric measures of non-compacted (NC) to compacted (c) myocardial length and mass ratios.INTRODUCTION
In pediatric population it is highly important to differentiate patients with pathologic left ventricular noncompaction (LVNC) who require regular surveillance and likely activity restriction, from those who are within the range of physiologic variant of hypertrabeculation and should not be activity restricted. Left ventricular noncompaction (LVNC) has possible major cardiac clinical manifestations such as congestive heart failure, arrhythmias, thromboembolism, and sudden cardiac death [1, 2], thus it is critical to identify these patients that require regular surveillance and likely activity restriction. Although MRI can reveal the non-compacted trabeculation (NC) distinctly from compacted myocardium (C), the current diagnostic criterion based on one dimensional measurements (NC/C>2.3) suffers from subjective variability and tend to over-diagnose left ventricular non-compaction (LVNC), especially in pediatric patients where LV trabeculation varies on a continuous spectrum [3].METHODS
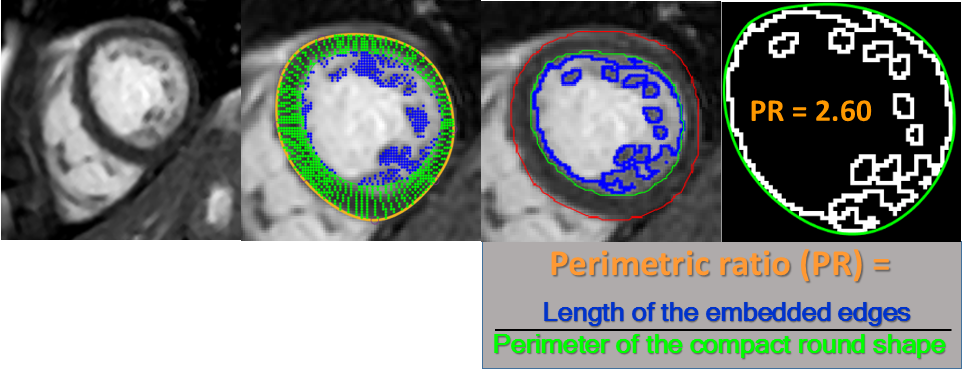
We retrospectively reviewed charts of patients who underwent cardiac MRI between August 2014 and September 2018 for clinical indications of hyper trabeculation, LV non-compaction, as well as patients with structurally normal cardiac anatomy such as anomalous coronary origins, or Kawasaki disease. Patients with normal structural anatomy, preload, and afterload conditions at the time of MRI were included in this study. Epi and endocardial contours (EC) were drawn on the end-diastolic short-axis bSSFP images of the LV from mitral valve annulus to apex (Fig. 1). These contours were used for automatic extraction of the trabecular edges (T). The following quantitative indices were computed using automated tool: 1) NC/C length ratio (LR) perpendicular to EC at each slice; 2) MR = percent NC of (NC+C) for entire LV; and 4) perimetric ratio (PR = length of T / perimeter of EC) for each slice. Global quantitative indices were derived as: 1) maximum of LR (MLR) across all slices; 2) MR; and 4) CPR over all slices. Combined criteria of MLR>2.3 and MR>35% was used to define patients with prominent trabeculations with possible LVNC.RESULTS
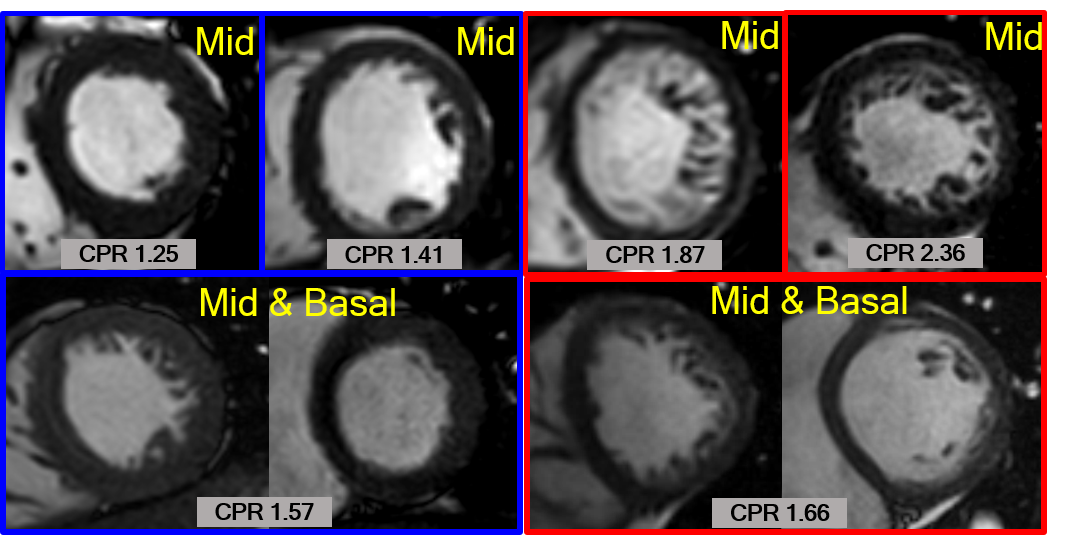
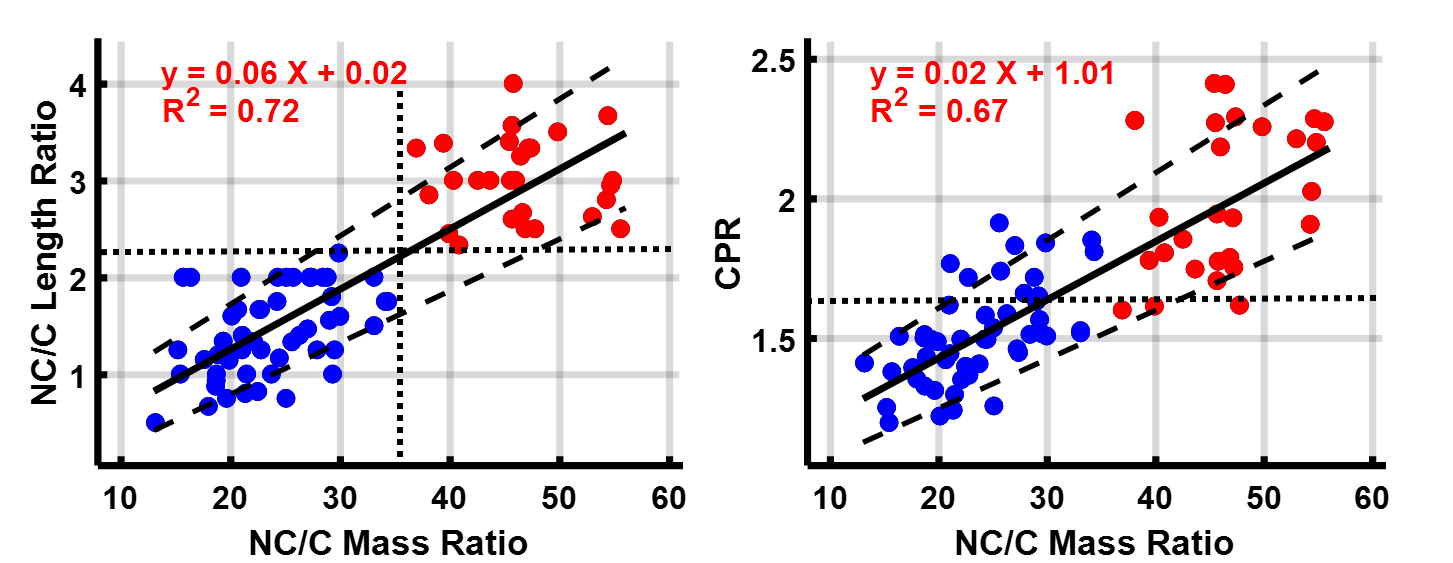
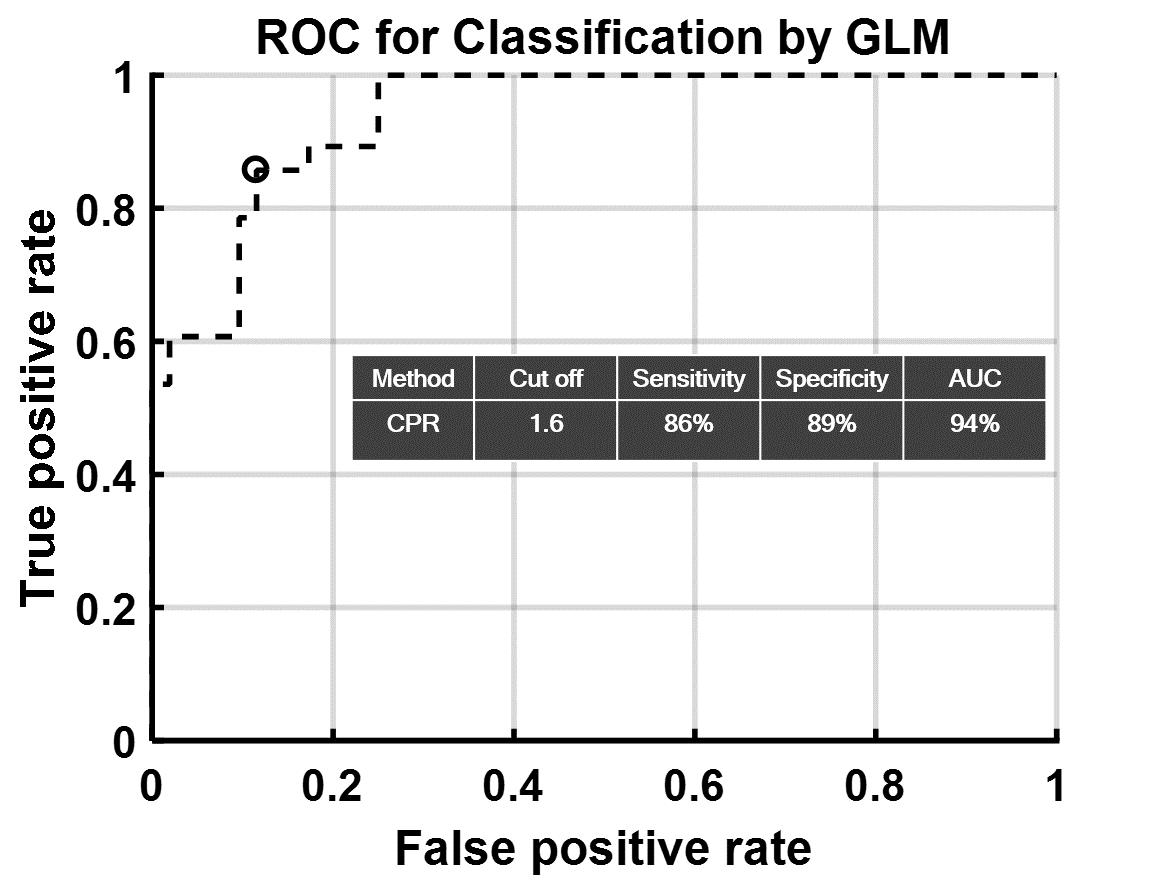
A total of 80 patients (14.3±5.0 yrs) met the inclusion criteria. Representative clinical images for the spectrum of degree of LV myocardial trabeculation with the resultant CPR values are shown in Figure 2. The values for MLR (1.99±0.88, 0.5-4), MR (31.7±12.1, 13.2-55.6), and CPR (1.67±0.31, 1.20-2.41) increased with degree of trabeculation as a continuous spectrum (Fig. 3). There is a significant correlation between MR and MLR with correlation coefficient (r) of 0.85 (0.78-0.9). CPR has significant correlation with both MLR (0.73, 0.61-0.82) and MR (0.82, 0.73-0.88). A total of 28 patients (15.3±5.5 yrs) met the criteria for prominent trabeculations. Cut off value of CPR=1.6 yields 94% of area under the receiver operating characteristics curve with 86% sensitivity and 89% specificity for identification of patients with prominent trabeculations (Fig 4).DISCUSSION & LIMITATIONS
Cumulative perimetric ratio captures the structural complexity (irregularity and sparsity) and extent of the LV myocardial trabeculation. CPR provides comprehensive measure of irregularity and extent of the LV trabeculations as it assimilates the inherent morphologic variation in structural complexity of LV trabeculation from base to apex. Effects of structural complexity and extent of myocardial trabeculation are amalgamated in CPR, thus it can distinguish between non-compaction and hyper-trabeculation. CPR does not take into account associated myocardial thinning which is crucial in settings of dilated cardiomyopathy and LVNC.CONCLUSION
In this study we described cumulative perimetric ratio as a novel index to summarily quantify the degree of LV myocardial trabeculations. CPR derived from epi and endocardial contours routinely drawn for LV functional analysis correlated strongly with morphometric measures of NC/C length and mass ratios. CPR has a potential to serve as a valuable biomarker for a quick quantitative assessment of degree of LV myocardial trabeculation. Furthermore, CPR can serve as a potential indicator for further assessment for LVNC with other established diagnostic tests.Acknowledgements
No acknowledgement found.References
[1] Rigopoulos A, Rizos IK, Aggeli C, Kloufetos P, Papacharalampous X, Stefanadis C, et al. Isolated left ventricular noncompaction: an unclassified cardiomyopathy with severe prognosis in adults. Cardiology. 2002;98:25–32.
[2] Stöllberger C, Blazek G, Dobias C, Hanafin A, Wegner C, Finsterer J. Frequency of stroke and embolism in left ventricular hypertrabeculation/noncompaction. Am J Cardiol. 2011;108:1021–3.
[3] Petersen SE, Selvanayagam JB, Wiesmann F, Robson MD, Francis JM, Anderson RH, et al. Left ventricular non-compaction: insights from cardiovascular magnetic resonance imaging. J Am Coll Cardiol. 2005;46:101–5.
Figures