2130
Left-atrial global longitudinal strain as an imaging biomarker of cardiac amyloidosis1University of Michigan, Ann Arbor, MI, United States, 2Medical College of Wisconsin, Milwaukee, WI, United States
Synopsis
Cardiac amyloidosis (CA) is a clinical disorder that could result in early death. MRI is a valuable modality for diagnosis of CA, where late-gadolinium enhancement is typically used for assessing adverse outcomes. However, in the era of unknown long-term effects of the gadolinium, there is a need to investigate alternative imaging biomarkers associated with CA, which is the primary aim of this study. The secondary aim is to evaluate the association between MRI variables and mortality in CA. The results demonstrated that depressed left-atrial global longitudinal strain is significantly associated with biopsy-proven CA, independent of other MRI and clinical measures.
INTRODUCTION
Cardiac amyloidosis is a clinical disorder caused by extracellular deposition of insoluble fibrils (approximately 7.5-10 nm wide) with beta-pleated sheet configuration [1]. Cardiac involvement can occur as part of a systemic disease or as a localized phenomenon, which could result in early death [2-3].
MRI is a valuable modality for diagnosis of cardiac amyloidosis (CA), where late gadolinium enhancement (LGE) is typically used for assessing adverse outcomes [4]. Nevertheless, with increasing awareness of the side effects of gadolinium-based contrast agents, there is a need to investigate alternative imaging biomarkers, especially those associated with altered heart mechanics, which are associated with CA.
Different MRI techniques have been developed for evaluating heart mechanics, e.g. MRI tagging [5], SENC [6], and DENSE [7]. Nevertheless, these techniques require special imaging pulse sequences and complicated post-processing techniques. Recently, MRI Feature Tracking (FT) has been introduced as a fast technique for evaluating heart mechanics from the cine images [8-9], which are typically acquired in almost all cardiac MRI exams; thus providing valuable measures of myocardial deformation, e.g. strain, without increasing the scan time.
In this study, we investigate the significance of myocardial strain, measured using MRI-FT, as an imaging biomarker associated with CA, beyond LGE, which is the primary aim of this study. The secondary aim is to evaluate the association between MRI variables and mortality in CA.
METHODS
Twenty patients (5 women and 15 men), age (mean ± standard deviation (SD)) of 61±13 y.o. with clinical suspicion for CA, who were referred to MRI and underwent cardiac biopsy, were included in the study. All patients were followed to date to evaluate for mortality.
The MRI exam consisted of: 1) cine images (a stack of parallel short-axis (SAX) slices covering the heart, in addition to four-chamber, two-chamber, and left-ventricular outflow-tract long-axis (LAX) images); and 2) LGE images at the same locations of the cine images. The cine imaging parameters were as follows: SSFP pulse sequence, TR=3.1ms, TE=1.55ms, flip angle=50⁰, Matrix=256x256, slice thickness=8mm, and bandwidth=1127Hz/pixel. The LGE imaging parameters were as follows: TR=6ms, TE=3ms, flip angle=25⁰, Matrix=256x256, slice thickness=8mm, and bandwidth=249Hz/pixel. TI was adjusted based on a Look-Locker sequence to null signal from normal myocardium.
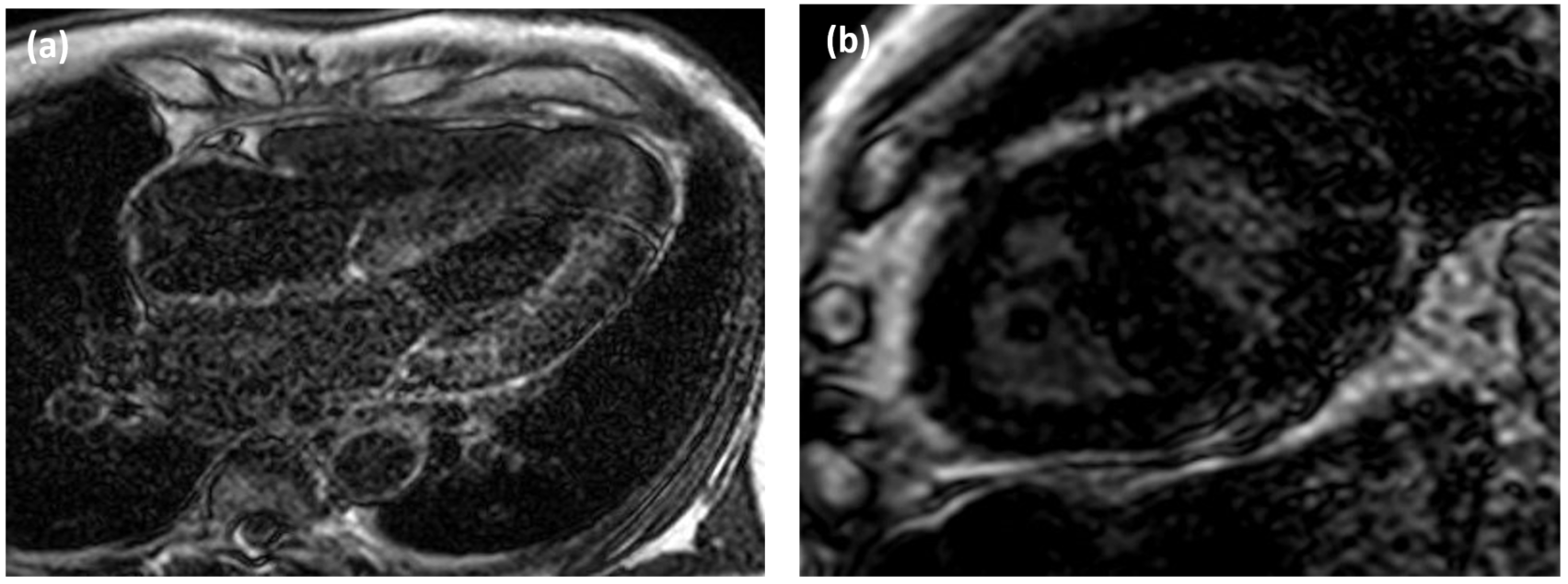
The MRI images were analyzed using Medis software. The cine images were semi-automatically processed using the QMass module to identify endocardial and epicardial contours at both end-systole and end-diastole timepoints, from which indexed left ventricular (LV) mass, ventricular volumes, and ejection fraction (EF) were measured. The Medis Feature-Tracking module was used to measure global ventricular and left-atrial (LA) strain. The LGE images were also analyzed using the QMass module to assess myocardial amyloid deposition (Figure-1).
Statistical univariate and multivariate logistic regression analysis, adjusted for cardiovascular disease risk factors, was performed to identify MRI measures that are associated with CA and mortality (p<.05 was considered significant).
RESULTS
Twelve out of the twenty patients (60%) were diagnosed with CA based on biopsy results. Ten patients (50%) had systemic light chain amyloidosis, 9 of whom had CA. The remaining 3 patients had transthyretin CA. Nine out of 13 patients that demonstrated LGE were diagnosed with CA, whereas the remaining 4 were not.
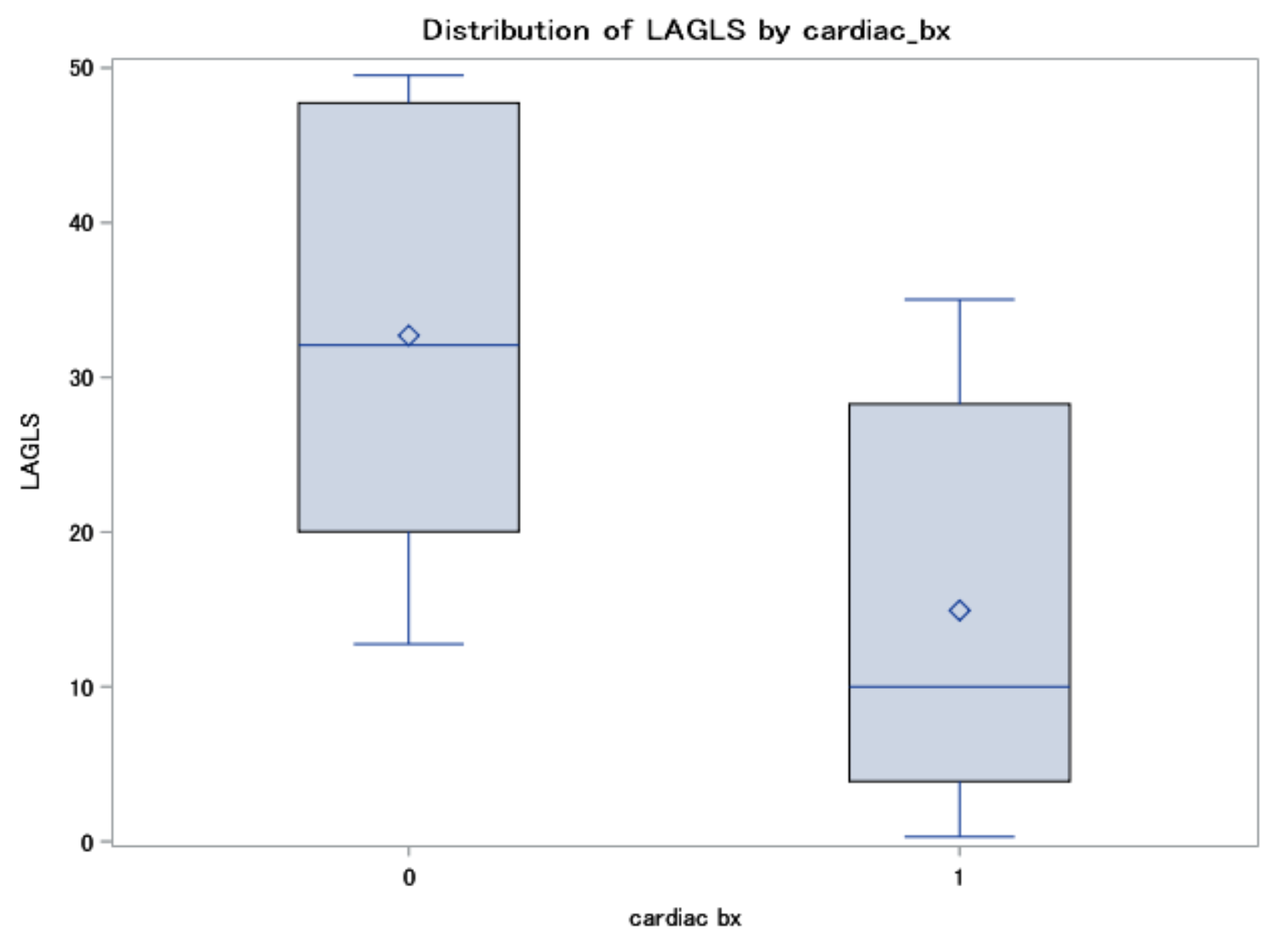
Patients with CA had significantly depressed left-atrial global longitudinal strain (GLS) than patients with no CA (mean±SD = -15±12% versus -33±13%, p=.01). In a multivariable analysis adjusted for cardiovascular disease risk factors, only LA GLS remained significantly associated with CA (p=.03) (Figure-2), while LGE was not (p=.48), as shown in Table-1. Seven out of nine patients who died were diagnosed with CA. However, none of the MRI and clinical variables were significantly associated with patients’ mortality.
DISCUSSION and CONCLUSION
The results demonstrated that depressed LA GLS is significantly associated with biopsy-proven CA, independent of other MRI and clinical measures.
Global strain measurement by feature tracking MRI has a number of advantages compared to other heart mechanics analysis techniques, including: 1) it does not require special acquisition sequences that add to the scan time; 2) post-processing is simple and fast; and 3) it does not need contrast agent administration. Specifically, the lack of the need for gadolinium injection is a big advantage as current trend in MRI is to adopt more gadolinium-free imaging sequences due to safety concerns and upcoming reports about contrast agent deposition in different body organs. This is of course in addition to inability to use gadolinium in patients with borderline kidney function or low glomerular filtration rate (GFR).
In conclusion, LA GLS has the potential to be a surrogate non-invasive imaging biomarker for evaluating cardiac amyloidosis beyond the need for LGE imaging.
Acknowledgements
No acknowledgement found.References
1. Merlini et al, J Intern Med; 255:159-178
2. Selvanayagam et al, J Am Coll Cardiol; 50:2101-2110
3. Desai et al, Cardiol Rev; 18:1-11
4. Nucifora et al, J Physiol Heart Circ Physiol; 307:H680-H688
5. Axel et al, Radiology; 171:841-845
6. Osman et al, Magn Reson Med; 46:324-334
7. Aletras et al, Magn Reson; 140:41-57
8. Maret et al, Cardiovasc Ultrasound; 7:53
9. Andre et al, J Cardiovasc Magn Reson; 16(Suppl 1): P321
Figures