2128
Automated Image Quality Assessment in 5D Whole-Heart MRI Aimed at Guiding Readers of High-Dimensional Dynamic Imaging1Department of Radiology, University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 2Advanced Clinical Imaging Technology, Siemens Healthcare AG, Lausanne, Switzerland, 3Center for Neuroprosthetics/Institutes of Bioengineering and Electrical Engineering, École Polytechnique Fédérale de Lausanne (EPFL), Lausanne, Switzerland, 4Center for Biomedical Imaging (CIBM), Lausanne, Switzerland, 5LTS5, École Polytechnique Fédérale de Lausanne (EPFL), Lausanne, Switzerland
Synopsis
A neural network trained to assess the quality of whole-heart coronary MRA images acquired with a respiratory self-navigated ECG-triggered bSSFP sequence was tested on images from a similar, but continuous non-ECG-triggered counterpart. Since cardiac and respiratory motion-resolved reconstructions of such acquisitions oftentimes consist of up to 150 individual 3D volumes, it is desirable to be able to automatically identify the volume with highest image quality for initial display to the reader. We found that the best image quality according to the neural network agreed with human visual assessment and was found in volumes corresponding to cardiac resting phases at end-expiration.
Introduction
Coronary Magnetic Resonance Angiography (CMRA) is conventionally gated to end-expiration and triggered to a cardiac resting phase in order to freeze motion.1 Recently, continuous non-ECG-triggered free-breathing sequences2, 3 that capture both the coronary anatomy and cardiac function have been proposed in order to improve the scan efficiency and ease of use. In the XD-GRASP4 approach to continuous CMRA that resolves both cardiac and respiratory motion5, the acquired data is subdivided into motion-state-consistent bins before reconstruction. The reconstructed dataset might consist of 15-25 different cardiac phases at 4-6 different respiratory levels; hence in total 60-150 3D volumes. In clinical practice, it would be cumbersome for the reader to visually decide which of the many volumes best answers to the clinical question at hand. Therefore, we aim at using automated image quality assessment to determine how the image quality varies within such 5D cardiac and respiratory motion-resolved reconstructions and to automatically identify volumes of high image quality to be proposed to the reader for initial examination.Methods
Automated image quality assessment was performed using an existing convolutional neural network (IQA-CNN).6 It had previously been trained to give Image Quality Scores (IQSs) ranging from 0 (non-diagnostic) to 4 (excellent) to images acquired using a prototype ECG-triggered respiratory self-navigated 3D radial bSSFP sequence7, 8. The datasets in this IRB-approved study were acquired with a continuous non-ECG-triggered version of the same sequence3 (Fig.1), providing similar contrast. Ten healthy subjects, who had provided written informed consent, were scanned on a 1.5T clinical MRI scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). Thereafter, the acquired datasets were reconstructed in a free-running framework for cardiac and respiratory motion-resolved imaging. Specifically, respiratory self-gating9 and the ECG were used for sorting the data into four respiratory levels that each resolved the cardiac cycle with a resolution of 50 ms prior to 5D (x-y-z-respiration-cardiac) XD-GRASP reconstruction5. Subsequently, two authors (DP and JH) visually ascertained which respiratory level provided the sharpest cardiac delineation as well as which systolic and diastolic volumes provided the best coronary conspicuity for each subject. In addition, the volumes corresponding to end-expiration and to the middle of systolic and diastolic resting phases were identified visually (LDS and JH). For automated assessment, the IQSs of all cardiac and respiratory phases were computed with the IQA-CNN. The best respiratory position for each subject was identified by averaging the IQSs over the cardiac dimension. Thereafter, the number of subjects where this corresponded to end-expiration was counted. Additionally, the number of instances where the maximum cardiac IQS at the best individual respiratory level matched the choice of at least one of the two readers was assessed. Finally, the average time from this cardiac IQS peak to the closest cardiac resting phase was computed over all subjects (temporal resolution limited to 50 ms).Results
Overall, the IQSs in the cardiac and respiratory motion-resolved datasets varied smoothly as a function of the respiratory and cardiac cycles (Fig.2). The volumes with best image quality according to the neural network was in good agreement with the human assessment, with the highest IQSs typically being assigned to volumes corresponding to end-expiration (Fig.3) and cardiac resting periods in both systole and diastole (Fig.4). In 8/10 subjects, end-expiration obtained the highest IQS. Moreover, in 9/10 subjects did the cardiac phase with maximal IQS correspond to the choice of at least one of the two readers. The average time from the cardiac phase with maximal IQS to a cardiac resting phase was 40±30 ms (0.8±0.6 phases).Discussion
The finding that the volumes corresponding to periods of minimal respiratory and cardiac motion obtained the highest IQSs is supported by the longstanding practice of targeting end-expiration and a cardiac resting phase in respiratory-gated ECG-triggered CMRA. Moreover, based on the agreement with the human readers, it appears that the IQA-CNN could be useful for reader guidance when handling a large number of reconstructed volumes. Since the human readers found it hard to pick single systolic and diastolic phases with maximal image quality (Fig.4), the volume with highest IQS would likely be a good choice to begin examining anatomy. Finally, it is encouraging that the IQA-CNN appears to provide meaningful results for images that were acquired with a continuous non-ECG-triggered version of the sequence that was used for training the algorithm.Conclusion
The image quality in the cardiac and respiratory motion-resolved datasets, as automatically scored by a convolutional neural network, was typically highest for the 3D volumes corresponding to end-expiration and cardiac resting periods. Moreover, the good agreement with human readers suggests that automated image quality assessment may be most useful in guiding the reader and improving the workflow in cases where large datasets have to be inspected.Acknowledgements
No acknowledgement found.References
1. M. R. Dweck, V. Puntman, A. T. Vesey, Z. A. Fayad, and E. Nagel, “MR Imaging of Coronary Arteries and Plaques,” JACC Cardiovasc. Imaging, vol. 9, no. 3, pp. 306–316, 2016.
2. J. Pang et al., “ECG and navigator-free four-dimensional whole-heart coronary MRA for simultaneous visualization of cardiac anatomy and function,” Magn. Reson. Med., vol. 72, no. 5, pp. 1208–1217, 2014.
3. S. Coppo et al., “Free-running 4D whole-heart self-navigated golden angle MRI: Initial results,” Magn. Reson. Med., vol. 74, no. 5, pp. 1306–1316, 2015.
4. L. Feng, L. Axel, H. Chandarana, K. T. Block, D. K. Sodickson, and R. Otazo, “XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing,” Magn. Reson. Med., vol. 75, no. 2, pp. 775–788, 2016.
5. L. Feng et al., “5D whole-heart sparse MRI,” Magn. Reson. Med., vol. 79, no. 2, pp. 826–838, 2018.
6. R. Demesmaeker et al., “Deep Learning for Automated Medical Image Quality Assessment : Proof of Concept in Whole-Heart Magnetic Resonance Imaging,” in Proceedings of the Joint Annual ISMRM-ESMRMB Meeting, 2018.
7. D. Piccini et al., “Respiratory Self-navigated Postcontrast Whole-Heart Coronary MR Angiography: Initial Experience in Patients,” Radiology, vol. 270, no. 2, pp. 378–386, 2014.
8. P. Monney et al., “Single centre experience of the application of self navigated 3D whole heart cardiovascular magnetic resonance for the assessment of cardiac anatomy in congenital heart disease.,” J. Cardiovasc. Magn. Reson., vol. 17, p. 55, 2015.
9. L. Di Sopra, D. Piccini, S. Coppo, J. A. M. Bastiaansen, M. Stuber, and J. Yerly, “Motion-Resolved 5D Imaging of the Heart: Time to Get Rid of the ECG?,” in Proceedings of the Annual ISMRM Meeting, 2017.
Figures
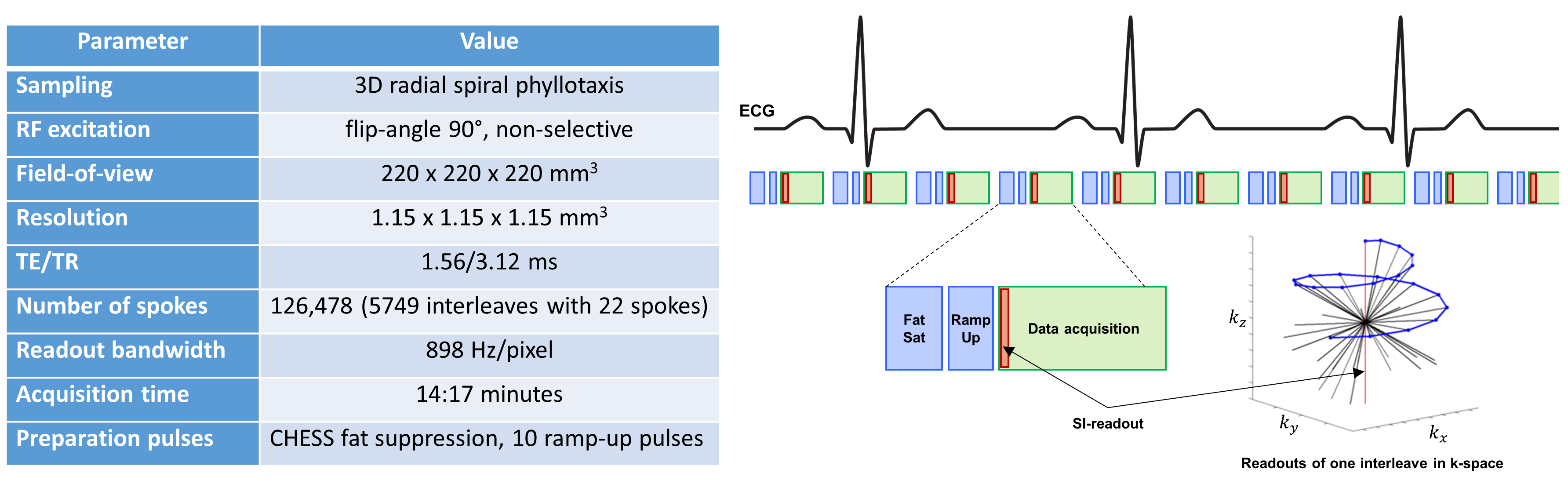
Figure 1. Sequence details
An overview of the respiratory self-gated free-breathing non-ECG-triggered golden angle 3D radial bSSFP sequence used in this study.
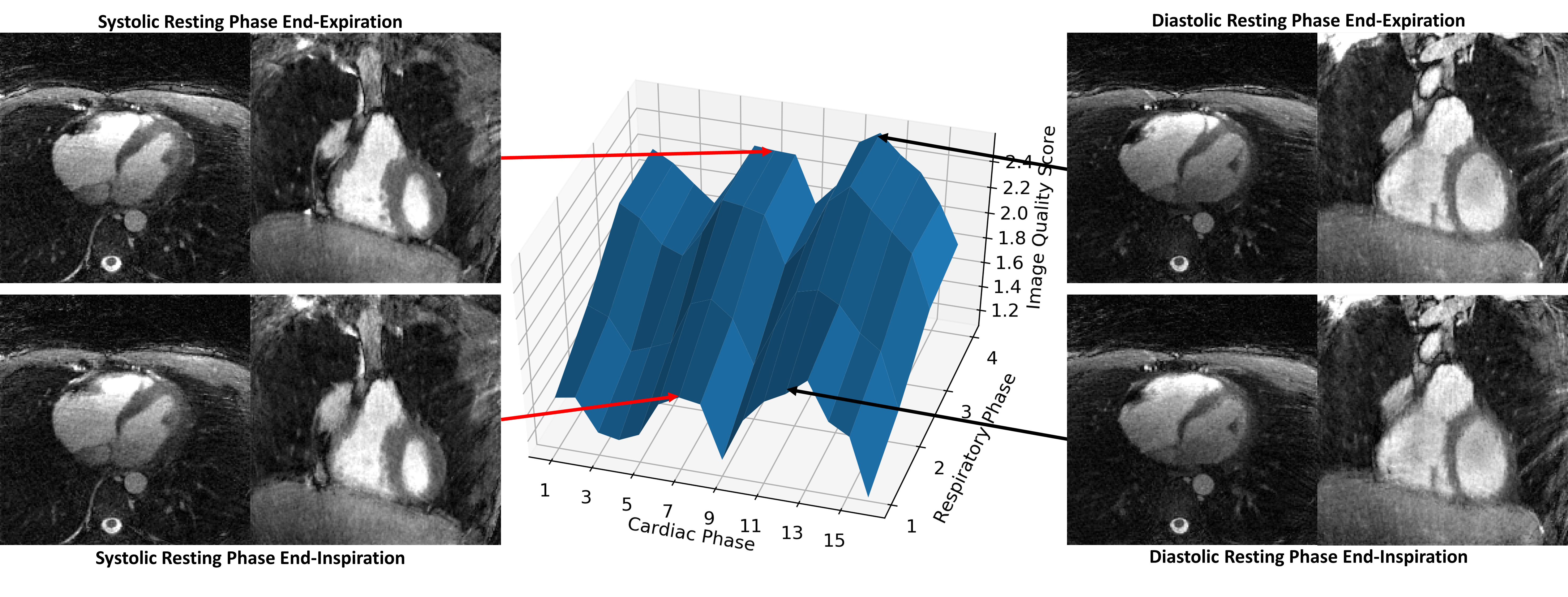
Figure 2. Example of image quality scores within a 5D dataset and corresponding images
Surface plot depicting the IQS distribution in a dataset with 4 respiratory phases and 16 cardiac phases. Notably, the image quality varies smoothly as a function of the cardiac and respiratory cycles. Moreover, the highest values coincide with end-expiration and the cardiac resting phases. Next to the surface plot, axial and coronal slices extracted from the isotropic 5D dataset at the cardiac resting phases in end-expiration and end-inspiration are shown.
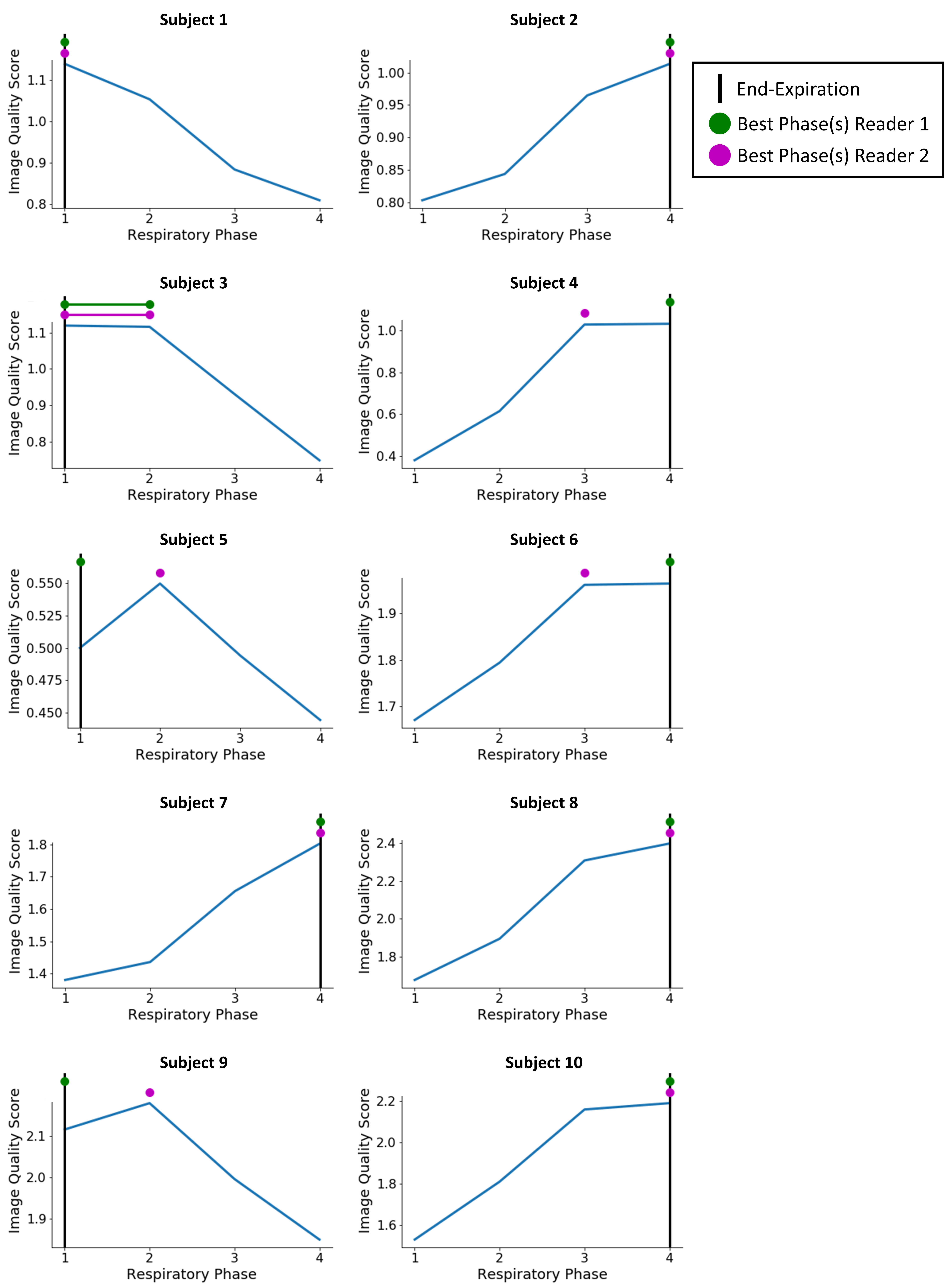
Figure 3. Image quality along the respiratory cycle
Plots showing the image quality scores of the different respiratory levels, computed as an average over all cardiac phases. The respiratory position that corresponds to end-expiration is marked with a vertical black line. Since the sign of the respiratory self-gating signals is arbitrary, end-expiration can correspond to either phase 1 or 4. In 8/10 subjects did end-expiration obtain the highest IQS. The green and purple disks correspond to the respiratory phases with best image quality according to the human readers. In subject 3, the readers considered two respiratory positions to be equivalent.
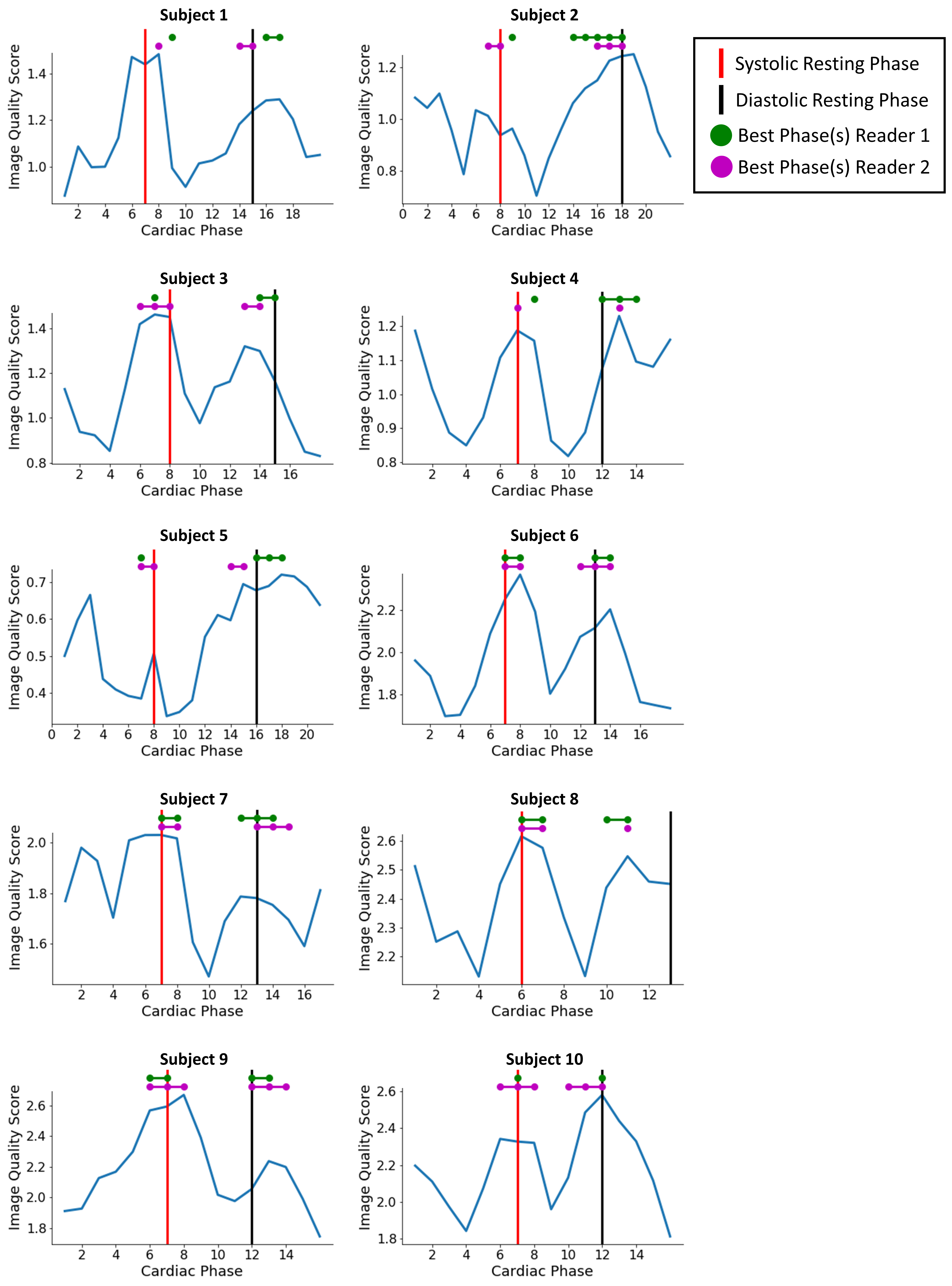
Figure 4. Image quality along the cardiac cycle
Plots showing the image quality scores of all cardiac phases of the subjects' best respiratory level. The systolic and diastolic resting phases are indicated with vertical red and black lines, respectively. The green and purple disks correspond to the cardiac phases with best image quality according to the human readers. In 9/10 subjects did the cardiac phase with maximum IQS correspond to the choice of at least one of the two readers. The average time from the cardiac phase with maximal IQS to a cardiac resting phase was 40±30 ms (0.8±0.6 phases).