2124
High Resolution Real-time Spiral Cine with Whole Heart Coverage in Under 30 Seconds1Department of Biomedical Engineering, University of Virginia, Charlottesville, VA, United States, 2School of Medicine, University of Virginia, Charlottesville, VA, United States
Synopsis
This study develops a spiral-in/out bSSFP pulse sequence combined with a low rank plus sparse (L+S) reconstruction method for free-breathing ungated high resolution real-time cine with whole heart coverage. Within 30 seconds, this proposed method achieves total ten slices spiral cardiac movies with an in-plane 1.37 x 1.37 mm2 spatial resolution and 40 ms temporal resolution.
Introduction
In clinical practice, cine images are typically acquired using breath-held ECG gated balanced steady-state free procession (bSSFP) pulse sequences. While producing images with high image quality and spatial/temporal resolution, this approach is time-consuming, typically taking 5-10 minutes, and may be affected by ECG-gating and breathing artifacts. Real-time cine pulse sequences1 are advantageous for patients with arrhythmias or difficulty holding their breath, yet typically suffer from reduced spatial and/or temporal resolution as compared to ECG-gated breath-held techniques. Recently, we introduced and compared two spiral-based (spiral-out and spiral-in/out) bSSFP sequences1, 2 for accelerated real-time cardiac MRI, and demonstrated that a spiral-in/out bSSFP sequence combined with an L+S reconstruction3 yields ungated cardiac movies with high image quality, minimal temporal blurring or off-resonance artifacts. However, this technique had relatively low spatial resolution. In this study, we modified our previously proposed method to acquire real-time spiral cine with high temporal (~40 ms), high spatial resolution (~1.4 mm spatial resolution) and spatial with whole heart coverage and in 30 seconds.Method
A schematic of the procedure is depicted in Fig.1. For each set of scans, sequential multi-slice acquisition was used to acquire ten slices. 480 spiral arms per slice were collected. A low spatial resolution field map per slice was acquired using two single-shot spirals before the bSSFP acquisition. Interleaved spiral-in/out readout with linearly decreasing sampling density from 1.2 to 0.4 was utilized in this study. The fully-sampled spiral trajectories contained 48 arms with 3.2 ms readout per arm, and eight interleaves 45o apart from each other were generated to reconstruct each cardiac phase with an undersampling rate of 6. The interleaves were rotated using a bit-reversed order to reduce the temporal correlation. FOV was set to 340 x 340 mm2, and TR was set to 5.02 ms. The total acquisition time for 10 slices was half a minute with 3 s per slice. Other sequence parameters and the resulting spatial and temporal resolutions are given in Table 1a.
The low rank plus sparse (L+S) algorithm was used for image reconstruction. The coil sensitivity was estimated from the center k-space data of the field map using ESPIRiT4 and then fed into the L+S kernel. The regularization parameters $$$\lambda_L$$$ and $$$\lambda_S$$$ were set to 0.05 and 0.003, respectively. The recent proximal optimized gradient method5 (POGM) was used for faster iterative convergence. Low resolution linear field maps and Chebyshev-based off-resonance correction6 methods were utilized for the L+S reconstruction method.
All experiments were performed on a 1.5T scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany) with a 32-channel surface coil array. For each healthy volunteer, whole heart coverage short-axis views were imaged both by the proposed method under ungated free-breathing conditions and by clinical ECG-gated cine technique during breath-holding as a reference.
Results and Discussion
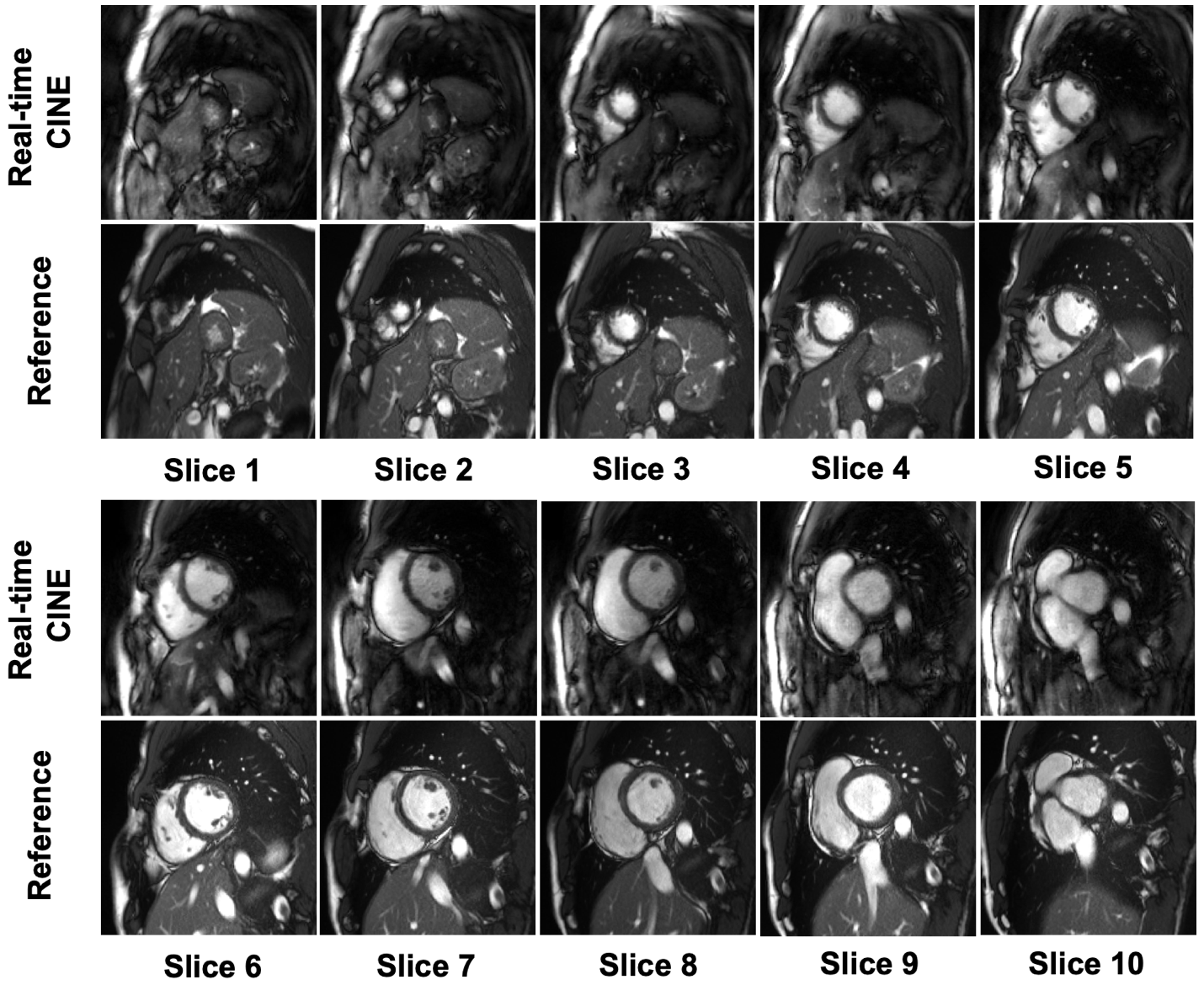
Whole heart coverage, short-axis dynamic image series from both the spiral-in/out bSSFP sequence and the clinical cine sequence are shown in Figs. 2 and 3. For the proposed method, a 6-fold acceleration is achieved, and a total of 60 frames per slice are reconstructed. Figs. 2 and 3 show systolic and diastolic frames of 10 slices acquired using the proposed real-time spiral cine method and the clinical reference method. The results show similar image quality for the two methods in systolic and diastolic frames, with somewhat lower image sharpness for the real-time method. Fig. 4 shows three frames at different phases along the cardiac cycle and the temporal profiles across the middle of left ventricle. The proposed method yields a relatively smooth transition between the end of systole and the end of diastole, when compared with the reference. Table 1b indicates the left ventricular ejection fraction estimates from three volunteers, and results from the proposed method are close to those from the reference.Conclusion
In this study, high resolution real-time cine with whole heart coverage was implemented and tested. The results show that within half a minute, the proposed method achieves 10-slice, ungated, free-breathing spiral cardiac movies at 1.37 x 1.37 x 8 mm3 spatial resolution and 40 ms temporal resolution per slice.Acknowledgements
No acknowledgement found.References
[1] Feng X, Salerno M, Kramer C M, Meyer CH. Non-Cartesian balanced steady-state free precession pulse sequences for real-time cardiac MRI. Magn Reson Med. 2016, 75(4):1546.
[2] Wang Z, Feng X, Dou Q, Meyer CH. Accelerated Spiral imaging for Real-time Cardiac MRI. Proceedings 26th Annual Meeting ISMRM, Paris. 2018:0935.
[3] Otazo R, Candes E, Sodickson DK. Low-rank plus sparse matrix decomposition for accelerated dynamic MRI with separation of background and dynamic components. Magn Reson Med. 2014. 73(3): 1125-1136.
[4] Uecker M, Lai P, Mruphy MJ, et al. ESPIRiT--an eigenvalue approach to autocalibrating parallel MRI: where SENSE meets GRAPPA. Magn Reson Med. 2014. 71(3): 990-1001.
[5] Lin CY, Fessler JA. Accelerated methods for low-rank plus sparse image reconstruction. IEEE 15th International Symposium on Biomedical Imaging, Washington. DC, 2018, pp. 48-51. doi: 10.1109/ISBI.2018.8363520
[6] Chen W, Sica CT, Meyer CH. Fast conjugate phase image reconstruction based on a Chebyshev approximation to correct for B0 field inhomogeneity and concomitant gradients. Magn Reson Med. 2008. 60(5): 1103-1111.
Figures