2120
Sex Differences in Type 2 Diabetes Mellitus-Related Left Ventricular Remodeling1Department fo Radiology, Zhongnan Hospital of Wuhan University, Wuhan, China, 2Department of Radiology, Southwest Hospital, Third Military Medical University, Chongqing, China, 3Siemens Healthcare, Shanghai, China
Synopsis
This
study aimed at demonstrate the influence of gender difference on T2DM related
LV structural, functional, as well as interstitial remodeling. Short-axis cine
imaging and pre- and post-contrast T1 mappings were analyzed in 62 T2DM
patients and 40 healthy controls. Significant LV concentric remodeling was noted
in female T2DM population while male patients exhibited extracellular matrix
remodeling and diastolic dysfunction.
Introduction
Type-2
diabetes mellitus (T2DM) can directly cause myocardial remodeling, typically
represented as a decreased left ventricular (LV) cavity, an increased LV wall
thickness, LV diastolic dysfunction and diffuse interstitial fibrosis, even in
the absence of hypertension and coronary artery disease.1 However, sex
difference in T2DM related LV structural, functional and interstitial
remodeling is not well described. Cardiac magnetic resonance (CMR) cine and T1
mapping have been widely used to characterize LV structure, function and
interstitial fibrosis. We aimed to explore the influence of sex on LV
remodeling patterns of T2DM by using CMR cine and T1 mapping.
Method
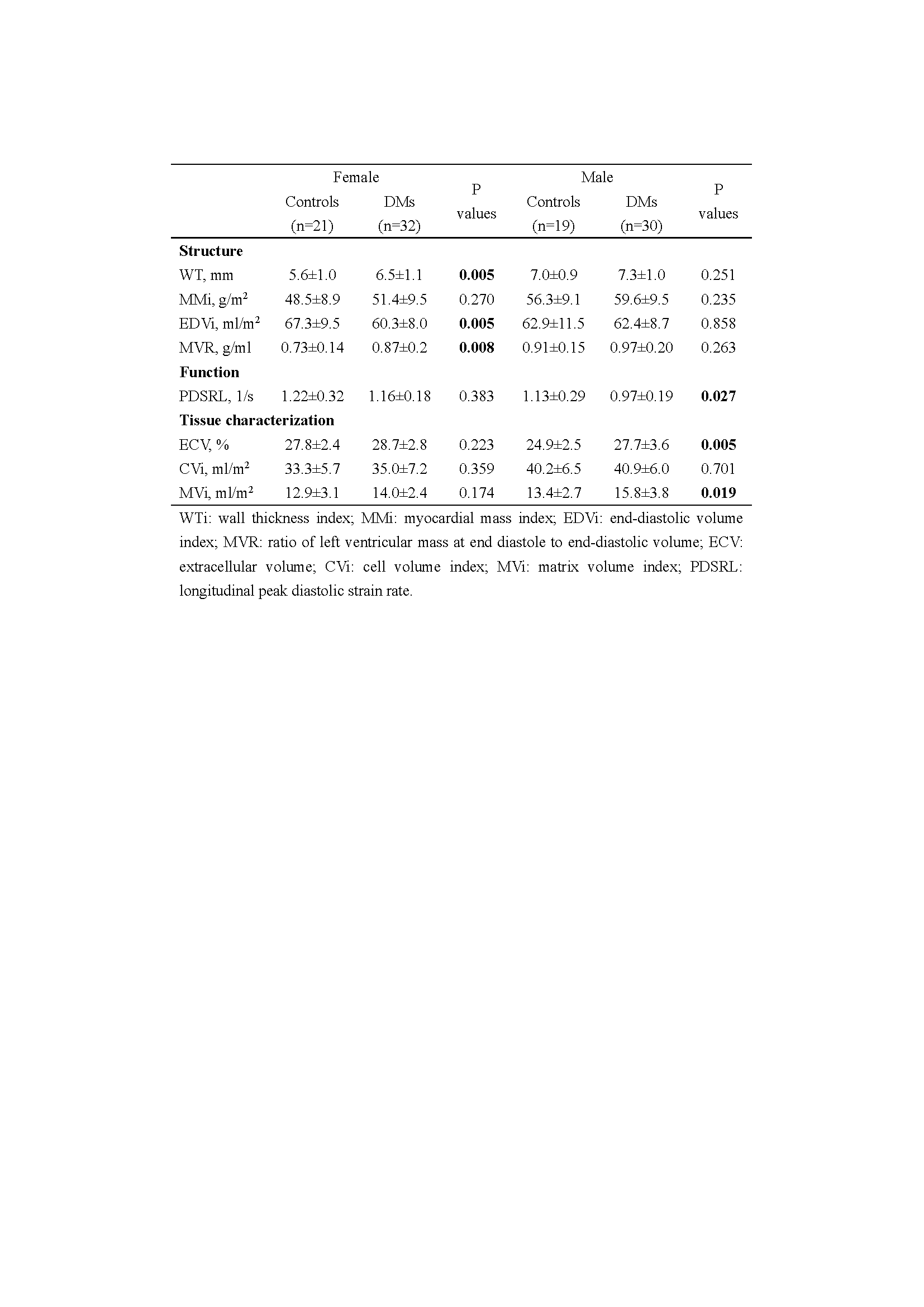
Sixty-two T2DM patients (32 females, age 55.7±8.0 years, T2DM duration 7(4-11) years; 30 males, age 53.5±7.9 years; T2DM duration 8(4-11.3) years) without history of cardiovascular disease or hypertension and 40 healthy controls (21 females, age 53±10.2 years; 19 males, age 47.7±13.1 years) were enrolled and underwent CMR on a 3T MR scanner (MAGNETOM Trio, Siemens Healthcare, Erlangen, Germany). Short-axis cine imaging covering the entire LV and long-axis cine in a standard four-chamber plane were performed using an electrographic (ECG)-gated, breath-hold steady-state free-precession (SSFP) sequence. Basal and mid-ventricular short-axis native and 15-min post-contrast T1 mappings were acquired using a breath-hold ECG-gated modified Look-Locker inversion recovery (MOLLI) prototype sequence with a 5b(3b)3b and 4b(1b)3b(1b)2b sampling pattern, respectively. Hematocrit was measured on the same day of the MR scan. All the cine and T1 maps were offline analyzed using the cvi42 software (Circle Cardiovascular Imaging Inc., Calgary, Alberta, Canada) to obtain the LV wall thickness, end-diastolic volume index (EDVi), myocardial mass index (MMi), the MMi-to-EDVi ratio (MVR), extracellular volume (ECV), total LV matrix and cell volumes index (MVi, CVi),2 and longitudinal peak diastolic strain rate (PDSRL).Results
Table 1 shows the alteration of LV structure, function and tissue characterization. Compared with male controls, female controls were accompanied by thinner wall thickness (p<0.001), smaller MMi (p=0.010), similar EDVi (p=0.191), smaller MVR (p<0.001) , similar PDSRL (p=0.349), smaller CVi (p=0.617) , similar MVi (p=0.001), and thereby larger ECV (p=0.001) than male participants. There were increased wall thickness (p=0.005), decreased EDVi (p=0.005), similar MMi (p=0.270) and CVi (p=0.359) in female T2DM compared to female controls, while, they were similar between male T2DM patients and male controls. T2DM male patients were accompanied by increased ECV (p=0.005) and MVi (p=0.019). However, there was no significant difference in ECV, CVi and PDSRL between female T2DM patients and female controls.Discussion&Conclusion
Acknowledgements
No acknowledgement found.References
1.Seferovic PM, Paulus WJ. Clinical diabetic cardiomyopathy: a two-faced disease with restrictive and dilated phenotypes. Eur Heart J 2015;36:1718-27.
2.Treibel TA, Kozor R, Fontana M et al. Sex Dimorphism in the Myocardial Response to Aortic Stenosis. JACC Cardiovasc imag 2018;11:962-973.
3.Levelt E, Mahmod M, Piechnik SK et al. Relationship Between Left Ventricular Structural and Metabolic Remodeling in Type 2 Diabetes. Diabetes 2016;65:44-52.
4.Wong TC, Piehler KM, Kang IA et al. Myocardial extracellular volume fraction quantified by cardiovascular magnetic resonance is increased in diabetes and associated with mortality and incident heart failure admission. Eur Heart J 2014;35:657-64.
Figures