2118
Inversion Recovery Cardiac and Respiratory Self-gated Simultaneous Acquisition of Cine and LGE Images Using a Golden-angle Spiral Pulse Sequence1Biomedical Engineering, University of Virginia, Charlottesville, VA, United States, 2Medicine, Radiology and Medical Imaging, University of Virginia, Charlottesville, VA, United States, 3Electrical and Computer Engineering, University of Virginia, Charlottesville, VA, United States, 4Electrical and Computer Engineering, University of Iowa, Iowa city, IA, United States, 5Medicine, Biomedical Engineering, Radiology and Medical Imaging, University of Virginia, Charlottesville, VA, United States
Synopsis
We proposed an inversion recovery respiratory and cardiac self-gated continuous spiral acquisition pulse sequence to acquire cine and LGE images simultaneously. Data is acquired using a single spiral interleaf, rotated by the golden-angle in time, with an inversion pulse applied every 5 seconds. Cine images were reconstructed from the steady state portion of the signal using L+S, while LGE images were reconstructed from the data at a specific TI after each inversion pulse using SPIRiT. This strategy will enable whole heart cine and LGE imaging in less than 5 minutes without the need for breath holding or ECG gating.
Introduction
In current clinical practice, breath-held ECG-gated short-axis cine images are typically acquired to assess cardiac function. At 10 minutes after injection of contrast agent, breath-held ECG-gated late gadolinium enhancement (LGE) images are separately acquired to characterize fibrosis. This routine is inefficient as it requires 10-12 breath-holds for cine imaging, and another 10-12 breath-holds for LGE. Further, it is susceptible to respiratory-motion artifacts and ECG gating artifacts, particularly at 3T. To overcome these shortcomings, we developed a continuous-acquisition strategy to simultaneously acquire both cine and LGE cardiac images post contrast during free breathing and without ECG gating.Methods
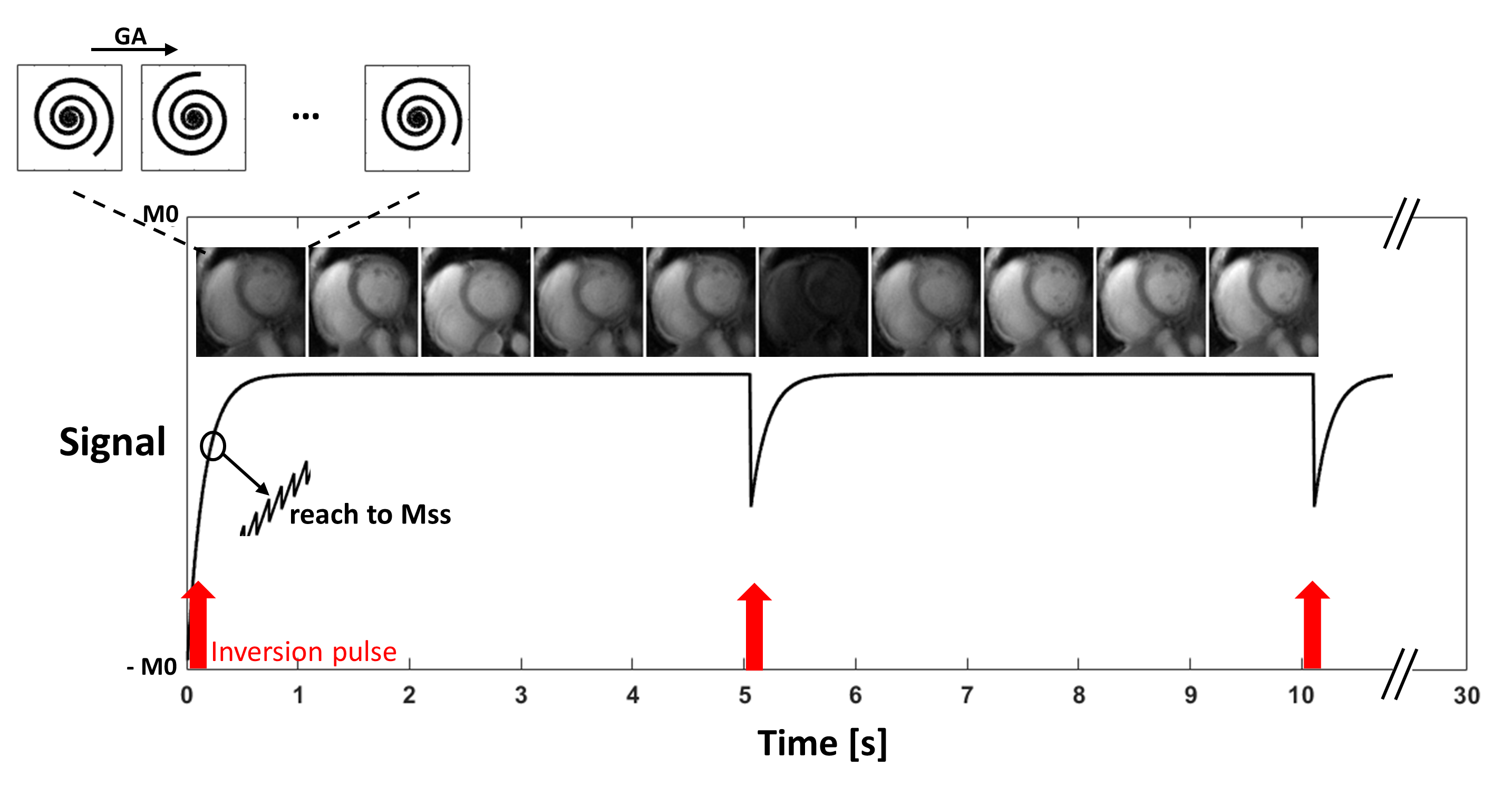
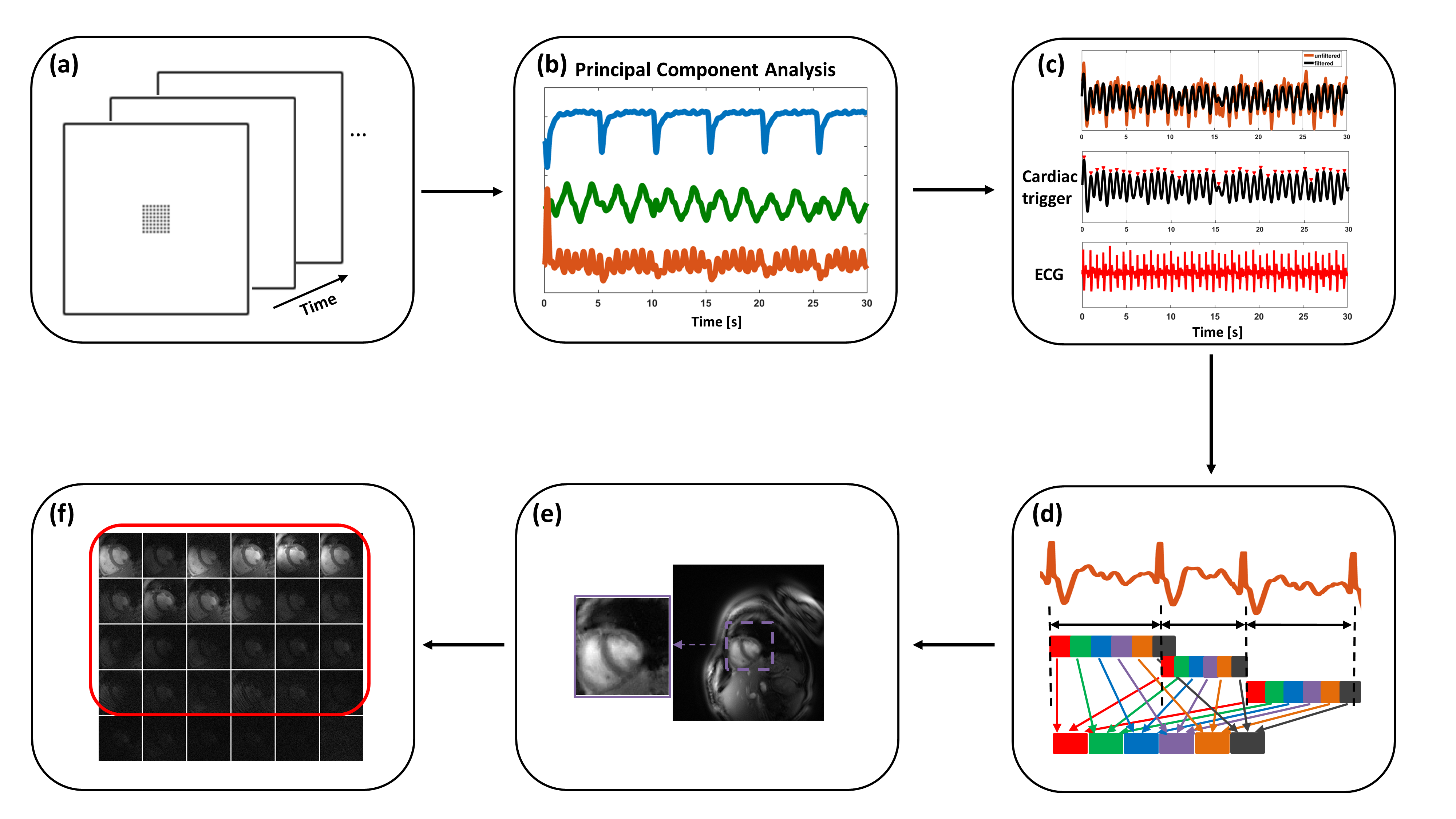
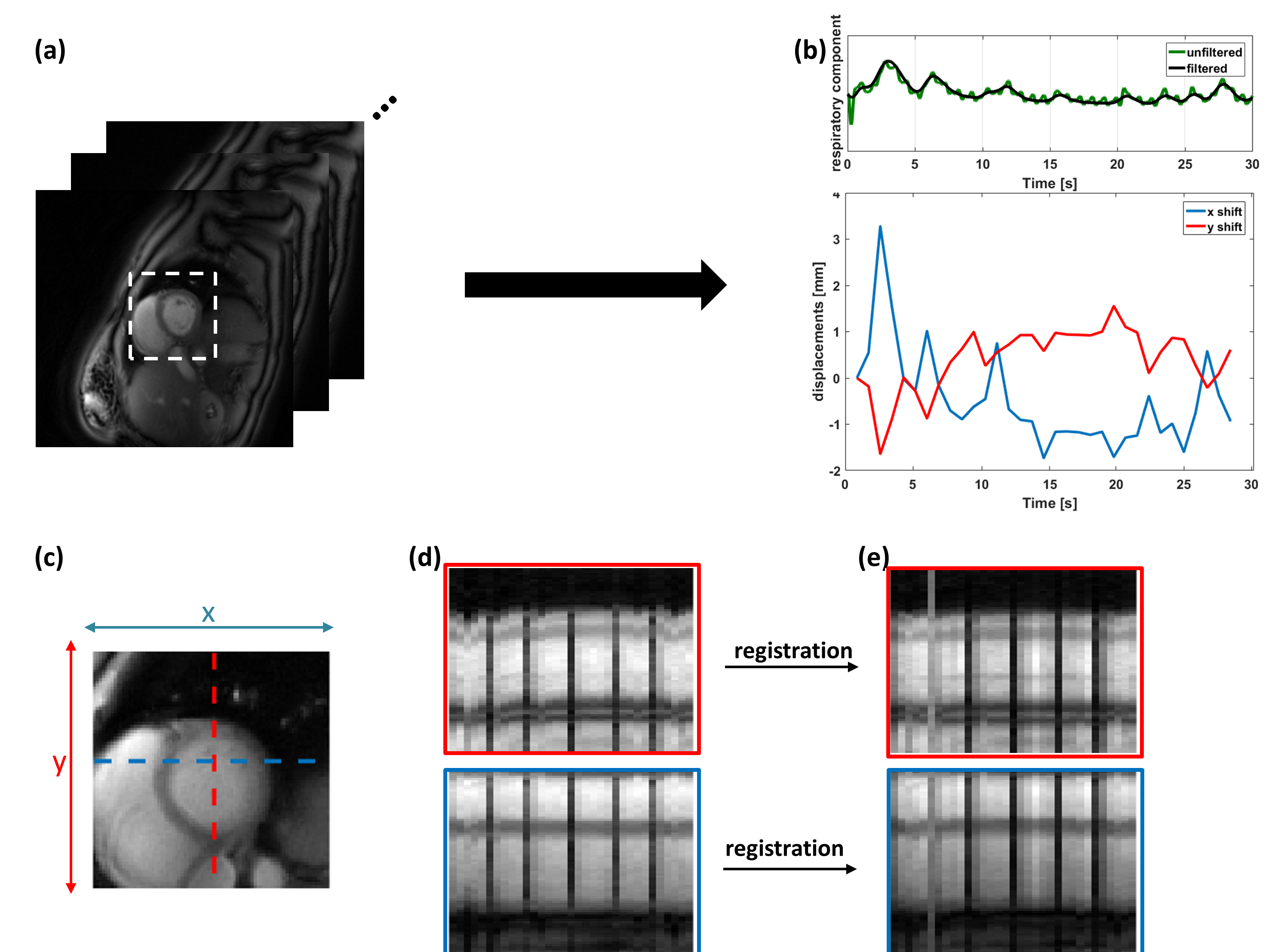
All in-vivo experiments were performed on a 3T scanner (Prisma, Siemens Healthineers). As shown in Figure 1, gradient echo data was acquired continuously for 30 seconds per slice using a pulse sequence consisting of a spiral trajectory rotated by the golden angle (GA). An adiabatic inversion pulse was applied every 5 seconds. Sequence parameters included: flip angle 15°, TR = 7.5 ms, TE = 1 ms, slice thickness = 8 mm, in-plane resolution = 1.5x1.5 mm2. Self-gating cardiac signals, the respiratory pattern, and the signal recovery curve following inversion recovery (IR) were extracted by gridding an 8x8 central region of k-space of each spiral interleaf for all coils (Figure 2a), followed by low-pass temporal filtering, principal component analysis (PCA) (Figure 2b), and band-pass filtering of the derived temporal-basis functions with peak detection (Figure 2c). The cardiac self-gating signal was used to retrospectively bin the data across the cardiac cycle (Figure 2d). An automatic algorithm was used to detect the heart 1 (Figure 2e) and select coils that had high SNR and minimal remote coil artifacts (Figure 2f). Breathing motion was corrected by reconstructing a static image using all spiral interleaves following each self-gating trigger for each heartbeat. Based on the heart region of interest (ROI), these images were rigidly-registered to derive and correct the respiratory motion for each RR interval 1 (Figure 3a).
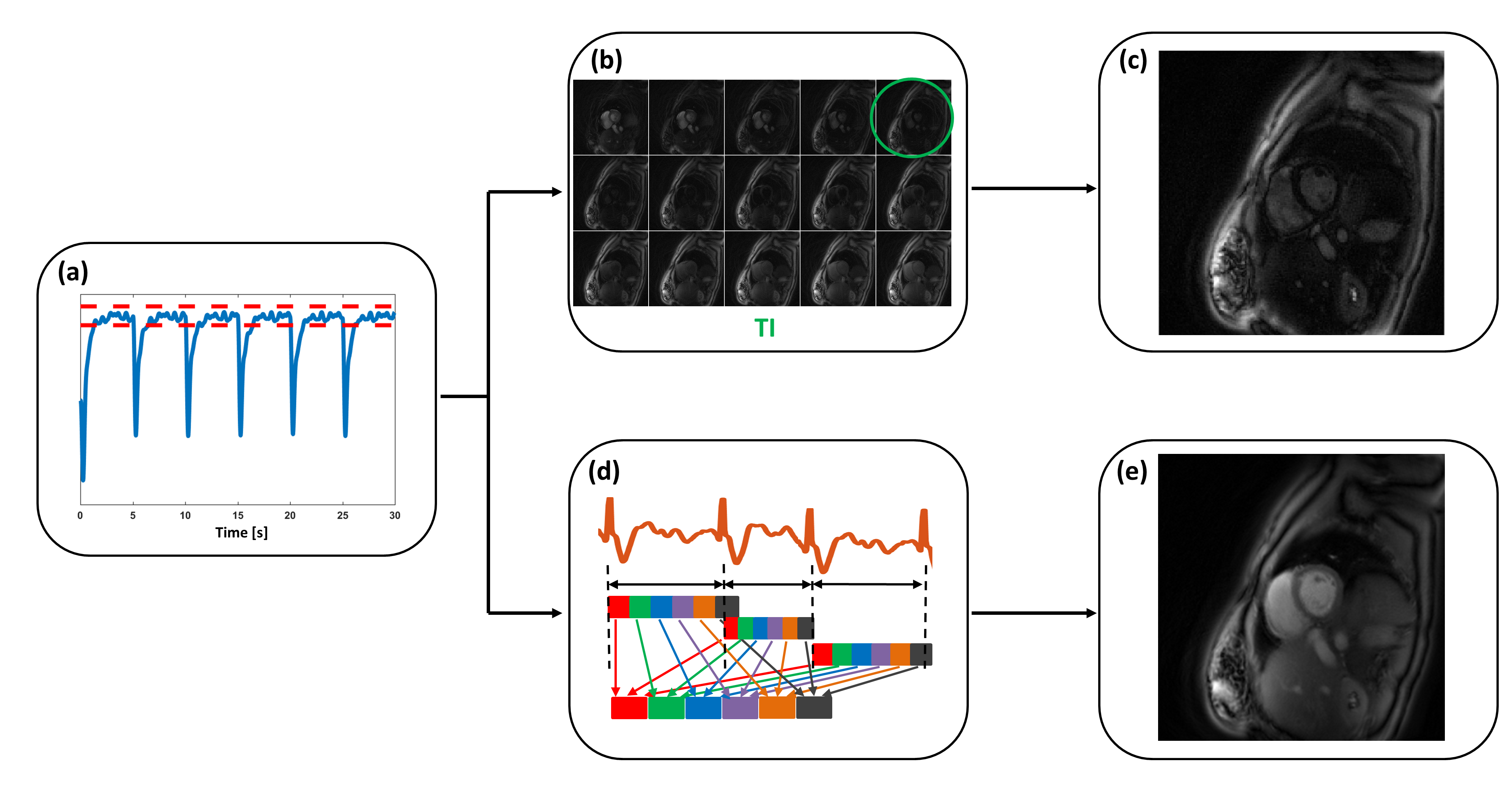
Using the signal recovery curve derived from PCA, a threshold was chosen based on the steady state signal across the data set (Figure 4a). The registered data was then separated into an LGE portion and a cine portion for image reconstruction. Cine images were reconstructed using low rank and sparsity (L+S) 2 after performing retrospective cardiac binning (Figure 4d) with a reconstructed temporal resolution of 38 ms (5 GA spirals/frame) (Figure 4e). For the LGE image, a sliding window approach was used in the first few hundred milliseconds after the 2nd inversion pulse to determine the inversion time (TI) (Figure 4b). Then the same cardiac phase data at the chosen TI after each inversion pulse (except the 1st one) were combined to reconstruct an LGE image using SPIRiT 3 with 150 ms temporal resolution (Figure 4c).
Results
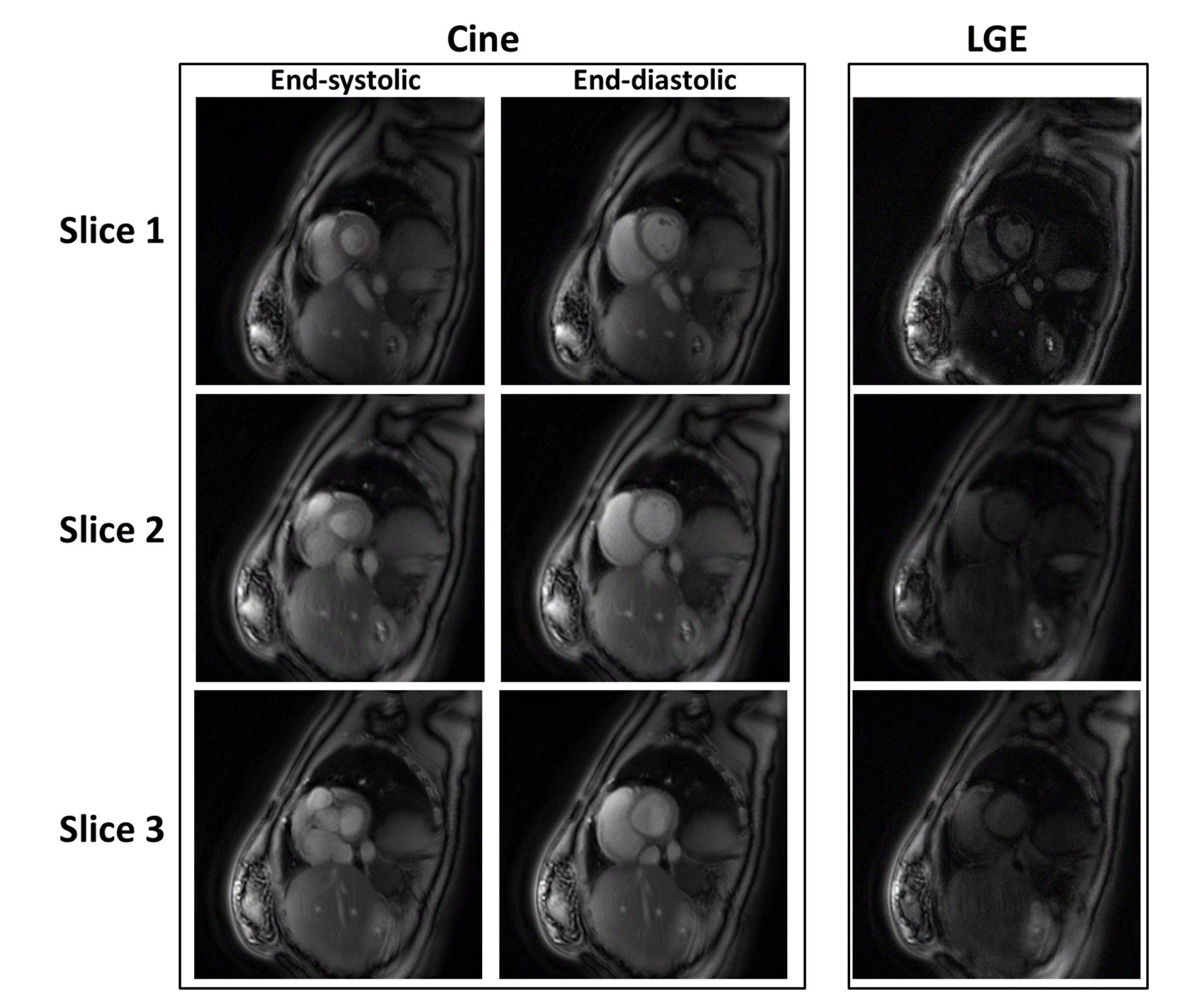
Figure 1 shows the general acquisition strategy used to simultaneously obtain cine and LGE images. After each inversion pulse, the signal intensity follows a T1* recovery curve. LGE images were obtained from data in the first few hundred milliseconds after each inversion pulse. Once the signal approaches steady state, cine images were generated. The derived cardiac trigger is consistent with the recorded ECG signal (Figure 2c). Figure 3 shows the rigid registration performance. X and y displacements are plotted in Figure 3b. The respiratory component extracted from PCA is also consistent with the respiratory signal derived from rigid registration. The registration performance can be seen by comparing the x-t (blue) and y-t (red) profiles before (Figure 3d) and after (Figure 3e) rigid registration. After registration, both x-t and y-t profiles are sharper and less corrupted by respiratory motion. Figure 5 shows the cine image results from one subject at diastolic and systolic phases of three short-axis slices, as well as the LGE image at the corresponding slices.Conclusion
Our simultaneous cine and LGE strategy with respiratory and cardiac self-gated acquisition demonstrates the feasibility of obtaining high quality cine and LGE images, with temporal and spatial resolution typical for breath-held cine imaging without the need for ECG gating or breath-holding. Performing LGE with self-gating completely removes the need for ECG-gating for cardiac magnetic resonance (CMR) viability studies. This strategy could greatly shorten the acquisition time and work for cine and LGE in clinical practice, providing a simpler, more efficient protocol for clinical CMR imaging particularly for patients who may have difficulty holding their breath. We aim to validate these techniques in patients with abnormal heart function and fibrosis.Acknowledgements
This work was supported by NIH R01 HL131919 and a grant from the Coulter Foundation.References
1. Zhou, R., Huang, W., et al. Simple motion correction strategy reduces respiratory-induced motion artifacts for k-t accelerated and compressed-sensing cardiovascular magnetic resonance perfusion imaging. J. Cardiovasc. Magn. Reson. 2018;20:1–13.
2. Otazo, R., Candès, E., Sodickson, D. K. Low-rank plus sparse matrix decomposition for accelerated dynamic MRI with separation of background and dynamic components. Magn. Reson. Med. 2015;73:1125–1136.
3. Lustig, M., Pauly, J. M. SPIRiT: Iterative self-consistent parallel imaging reconstruction from arbitrary k-space. Magn. Reson. Med. 2010;64:457–471.
Figures