2116
Sex Differences in Cardiac Biomechanics of Healthy Volunteers1Mechanical Engineering, University of Wisconsin-Madison, Madison, WI, United States, 2Radiology, University of Wisconsin-Madison, Madison, WI, United States, 3Medical Physics, University of Wisconsin-Madison, Madison, WI, United States, 4Cardiovascular Medicine, University of Wisconsin-Madison, Madison, WI, United States
Synopsis
The prevalence and prognoses of cardiac diseases differ between men and women due to a number of physiological factors. However, the implications of these differences on cardiac flow dynamics are not yet fully understood. In this study, healthy volunteers were imaged with four-dimensional flow and bSSFP MRI. Differences were observed between metrics of ventricular kinetic energy, ventricular flow vorticity, myocardial strain, and efficiency indices. Results may, in part, explain the hypothesized physiological protective effects of the pre-menopausal female heart, and their relevance to efficient cardiac flow dynamics.
INTRODUCTION
Traditionally, cardiovascular disease has been perceived as a greater threat to male health, and literature suggests that men are at greater risk for development of cardiovascular disease than age-matched pre-menopausal women.(2) However, the prevalence of ischemic heart disease (IHD) in women is high, as it causes approximately one third of all female deaths.(3,4) Furthermore, IHD is known to be more fatal in women and the incidence of general cardiovascular disease increases distinctly in women after menopause.(2,5) Nevertheless, the true causes and detailed mechanisms driving these differences are not fully understood.
A method that has recently gained traction in the evaluation of cardiac function is flow analysis with Four-dimensional (4D) flow magnetic resonance imaging (MRI). Of particular interest in recent studies is the amount of kinetic energy (KE) dissipation and flow vortex formation in healthy and diseased ventricles.(6-14) However, the differences between sexes in kinetic energy and vorticity metrics have not yet been thoroughly examined and related to cardiac function. Therefore, the purpose of this study was to analyze the ventricular flow dynamics and cardiac function of healthy volunteers and make comparisons based on sex.
METHODS
In this IRB-approved and HIPAA–compliant study, forty healthy volunteers (twenty-one men, nineteen women) were recruited. To date, eleven male subjects (age 26.7 ±, 3.2 years) and ten female subjects (age 26.2 ± 3.5 years) have completed the study. The subjects were scanned on a 3.0T clinical system (MR750, GE Healthcare) using a 4D Flow MRI sequence known as PC-VIPR.(15) Time-resolved flow data were reconstructed into 14 time frames per cardiac cycle. Data were imported to Ensight (CEI, Apex, NC), where flow metric measurements were made at the great vessels and ventricles for each time frame of the cardiac cycle. The KE within each ventricle was then quantified through analysis of the MR image data files and ventricular volumes using Matlab (Mathworks, Natick, MA). Efficiency indices, Reynolds number, and ventricular vorticities were also processed and computed in Ensight. Two-dimensional cardiac cine images were also obtained from each patient during the 4D flow MRI session. These images were used to calculate cardiac function and cardiac strain metrics using Segment (Medviso, Lund, Sweden) (http://segment.heiberg.se). Data were compared using a Student’s t-test and linear regression was used to determine the strength of correlations between measured parameters.RESULTS
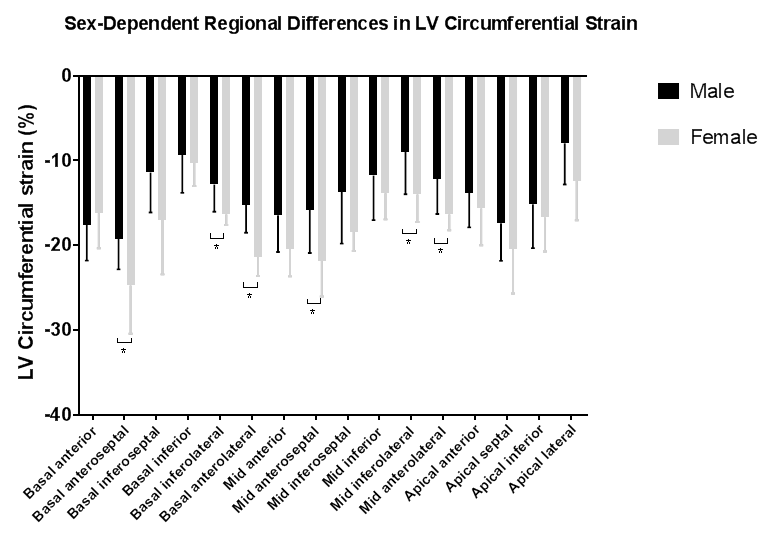
Averaged hemodynamic parameters for both male and female volnteers are plotted in Figure 2, while peak values are shown in Figure 3. Peak systolic kinetic energy was significantly higher in the left ventricle of men than it was in women (p=0.03). Additionally, peak LV efficiency index was higher in women than it was in men, although this result was not significant given the current sample size. On average, ventricular vorticity was higher in women than in men(p=0.003). Reynolds number was significantly correlated to vorticity in both men and women (Men: r=0.75, p=0.002; Women: r=0.59, p=0.026). Global circumferential LV strain (p=0.014), LV long-axis strain (p=0.001), and both base-(p=0.009) and mid-(p=0.015) left ventricle circumferential strain were significantly higher in women than in men, as shown in Figure 4. Furthermore, circumferential systolic (p=0.051) and diastolic (p=0.050) strain rates and long axis systolic (p=0.014) and diastolic (p=0.012) strain rates were significantly higher in women than in men. Differences in circumferential strain measurements are shown in figure 5.
DISCUSSION
The causes and effects of heart disease can be sex-dependent. It has been hypothesized that hormonal differences between sexes are the main drivers for the sex differences in cardiac function and disease progression. Literature suggests that estrogen can have a protective effect on the pre-menopausal female heart and leads to higher ischemia and reperfusion injury tolerance.(2) It has also been proposed that sex steroids have a significant influence on the contraction of cardiac myocytes and the regulation of autophagy during myocardial infarction.(2,5) However, the implications of these differences on the hemodynamic output of the heart are not yet understood. Through this study, it was observed that the male ventricle may be less efficient at producing flow than the female ventricle, due to higher kinetic energy dissipation, decreased myocardial strain, and less vorticity per amount of generated flow. Taken together, these augmentations in cardiac function in the female sex may in part explain the beneficial effects of estrogen. However, further studies will need to confirm the relationship between sex hormones and cardiac function.CONCLUSION
Observed sex-based differences in cardiac flow dynamics have potential implications on sex-specific causes and effects of heart disease. Such characteristics will be studied further in the remaining eighteen volunteers enrolled in this study.Acknowledgements
The research presented was supported by the NIH (UL1TR000427, TL1TR000429). The authors also wish to acknowledge support from GE Healthcare who provides research support to the University of Wisconsin.References
1. WorldHealthOrganization. 2017.
2. Kolar F, Ostadal B. Sex differences in cardiovascular function. Acta Physiol (Oxf) 2013;207(4):584-587.
3. Aggarwal NR, Patel HN, Mehta LS, et al. Sex Differences in Ischemic Heart Disease: Advances, Obstacles, and Next Steps. Circ Cardiovasc Qual Outcomes 2018;11(2):e004437.
4. Humphries KH, Izadnegahdar M, Sedlak T, et al. Sex differences in cardiovascular disease - Impact on care and outcomes. Front Neuroendocrinol 2017;46:46-70.
5. Le TY, Ashton AW, Mardini M, et al. Role of androgens in sex differences in cardiac damage during myocardial infarction. Endocrinology 2014;155(2):568-575.
6. Al-Wakeel N, Fernandes JF, Amiri A, et al. Hemodynamic and energetic aspects of the left ventricle in patients with mitral regurgitation before and after mitral valve surgery. J Magn Reson Imaging 2015;42(6):1705-1712.
7. Bermejo J, Benito Y, Alhama M, et al. Intraventricular vortex properties in nonischemic dilated cardiomyopathy. Am J Physiol Heart Circ Physiol 2014;306(5):H718-729.
8. Gürel E, Prinz C, Van Casteren L, Gao H, Willems R, Voigt JU. The Impact of Function-Flow Interaction on Left Ventricular Efficiency in Patients with Conduction Abnormalities: A Particle Image Velocimetry and Tissue Doppler Study. J Am Soc Echocardiogr 2016;29(5):431-440.
9. Han QJ, Witschey WR, Fang-Yen CM, et al. Altered Right Ventricular Kinetic Energy Work Density and Viscous Energy Dissipation in Patients with Pulmonary Arterial Hypertension: A Pilot Study Using 4D Flow MRI. PLoS One 2015;10(9):e0138365.
10. Jeong D, Anagnostopoulos PV, Roldan-Alzate A, et al. Ventricular kinetic energy may provide a novel noninvasive way to assess ventricular performance in patients with repaired tetralogy of Fallot. J Thorac Cardiovasc Surg 2015;149(5):1339-1347.
11. Kanski M, Arvidsson PM, Töger J, et al. Left ventricular fluid kinetic energy time curves in heart failure from cardiovascular magnetic resonance 4D flow data. J Cardiovasc Magn Reson 2015;17:111.
12. Pierrakos O, Vlachos PP. The effect of vortex formation on left ventricular filling and mitral valve efficiency. J Biomech Eng 2006;128(4):527-539.
13. Sjöberg P, Heiberg E, Wingren P, et al. Decreased Diastolic Ventricular Kinetic Energy in Young Patients with Fontan Circulation Demonstrated by Four-Dimensional Cardiac Magnetic Resonance Imaging. Pediatr Cardiol 2017;38(4):669-680.
14. Wong J, Chabiniok R, Pushparajah K, et al. Kinetic Energy Ejection Fraction: A Better Marker Of Cardiac Function In The Single Ventricle Circulation. Journal of the American College of Cardiology 2015;65(10).
15. Johnson KM, Lum DP, Turski PA, Block WF, Mistretta CA, Wieben O. Improved 3D phase contrast MRI with off-resonance corrected dual echo VIPR. Magn Reson Med 2008;60(6):1329-1336.
Figures




Figure 4. Comparison between metrics of myocardial strain. ). Global circumferential LV strain (p=0.014), LV long-axis strain (p=0.001), and both base-(p=0.009) and mid-(p=0.015) left ventricle circumferential strain were significantly higher in women than in men. Circumferential systolic (p=0.051) and diastolic (p=0.050) strain rates and long axis systolic (p=0.014) and diastolic (p=0.012) strain rates were significantly higher in women than in men