2115
Free-breathing left atrial volumetric cine imaging and strain mapping with interleaved radial, multi-band self-gating, UNFOLD, and parallel imaging1Yale University, New Haven, CT, United States
Synopsis
We developed a multi-slice free-breathing volumetric GRE cine imaging sequence for generating a 3D peak strain map for the left atrium. The sequence uses interleaved radial acquisition and a novel multi-band self-gating technique, accelerated with UNFOLD, and parallel imaging. The method was validated in 8 healthy subjects against alternative motion-correction methods. The results showed a stable performance using multi-band self-gating, and a sufficient image quality to generate a 3D strain map using feature tracking. This method provides a novel approach to interrogate the relationship between left atrial fibrosis, quantified by 3D left atrial gadolinium enhancement, and left atrial strain.
Purpose
The traditional method for evaluating left atrial (LA) strain with MRI is based on long-axis cine imaging(1,2), which has limitations in that the 3D deformation is not measured. Three-dimensional gradient-echo (GRE) cine in the left atrium has low SNR due to inflow oversaturation (3); standard 2D or 3D balanced SSFP atrial cine suffers from severe off-resonance artifacts characteristic of the pulmonary veins (4). We developed a multi-slice volumetric GRE cine imaging sequence with free-breathing, which is achieved by interleaved radial acquisition and a novel multi-band self-gating technique, accelerated with UNFOLD (5), and parallel imaging. The pseudo-3D cine data was used to generate 3D peak strain maps for the left atrium.Methods
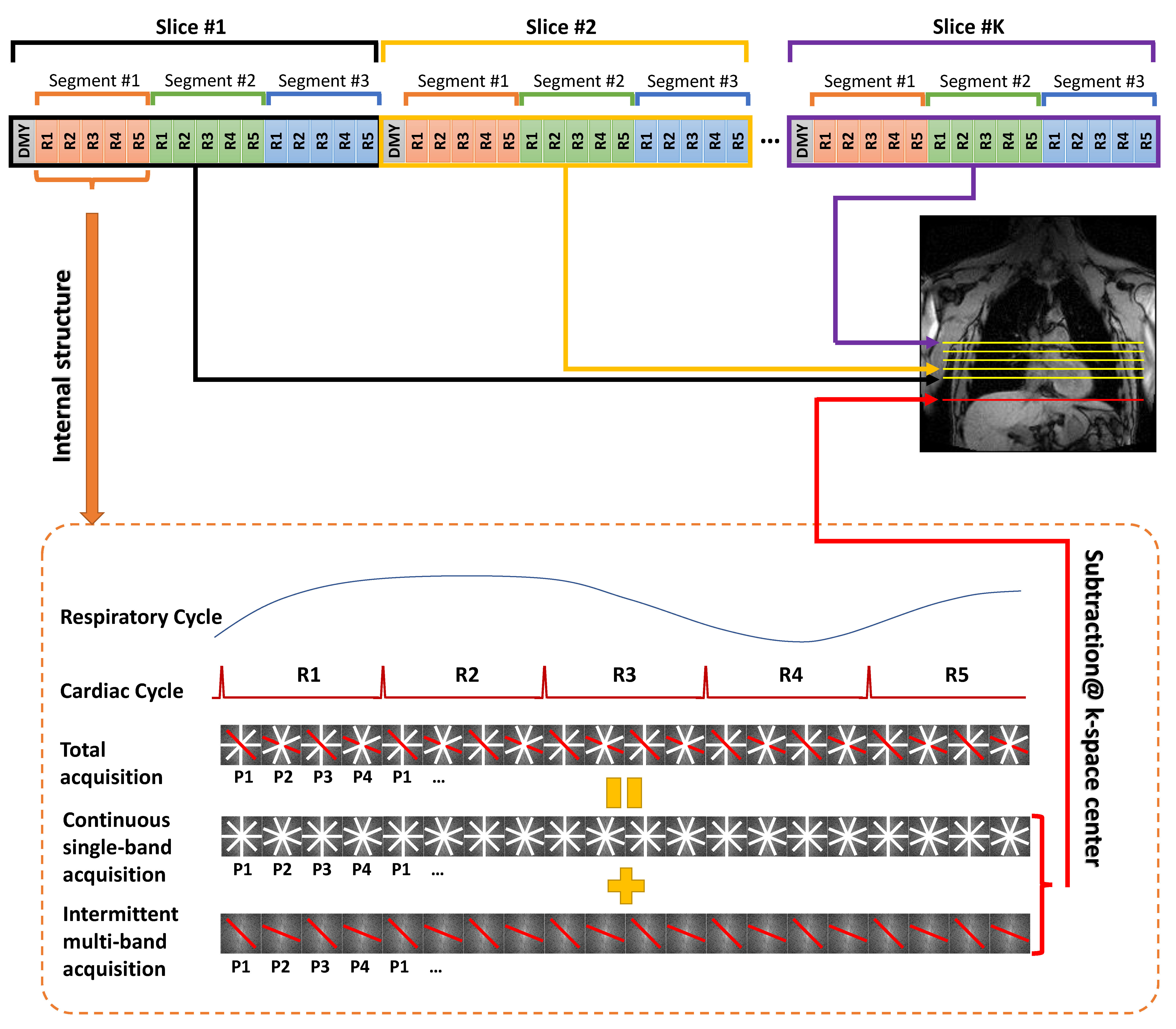
Volumetric cine imaging: The respiratory self-gated sequence cannot use standard methods (6,7), since the axial slices in the atrium do not contain respiratory information. An interleaved radial GRE cine sequence was thus modified to insert at each cardiac phase a multi-band RF pulse, which excites both the imaging slice and a parallel navigator slice located in the diaphragm (See Figure 1). The multi-band TR used the same flip angle as the previous TR, so that subtraction of the two signals generates a DC signal from the navigator-slice for self-gating. The steady state in both planes is maintained thanks to the multi-band self-gating. K-space sampling is interleaved and repeated multiple times for retrospective respiratory-gating. Respiratory bellows data was collected to validate the self-gating signal. Reconstruction was performed by firstly applying gridding and UNFOLD filtering to each channel. Iterative SENSE with l2-regularization was then performed to reconstruct the image at each phase.
Strain mapping: A 3D phase-resolved deformation field was obtained by recursively applying a 3D nonrigid registration algorithm (8) to each pair of neighboring phases, ranging from end-diastole (ED) to end-systole (ES). The total deformation field from ED to ES was then calculated by concatenating the phase-resolved deformation field. The LA end-diastolic cavity was manually contoured and triangularly meshed to generate a 3D LA model. The strain was calculated based on the change of area of each triangular element, using the following formula, assuming isotropic strain:
Strain=√(AreaES/AreaED) - 1
In vivo study: The study was IRB-approved, and all subjects provided written informed consent.Eight healthy subjects (age 30±10, 4 male) were scanned with the proposed method in a 3T scanner (Siemens Trio), with 14-16 axial planes covering the LA. The slice plane for the navigator was set at the diaphragm dome in end-inspiration, typically 30mm-60mm lower than the imaging planes. Fifty-one projections were acquired with 17 views per segment, with 4-7 repetitions for retrospective respiratory gating. Each phase lasts 62ms with asymmetric echo, and scan time was 4.5 minutes. Other parameters were: FOV/image size/slice-thickness/flip-angle/TR/parallel imaging/bandwidth = 300mm×300mm/192×192/4mm/15°/3.6ms/650Hz/pixel. A radial GRE cine sequence (single breath-hold, 195 radial projections) was also performed in a single slice, providing a gold standard for motion correction.
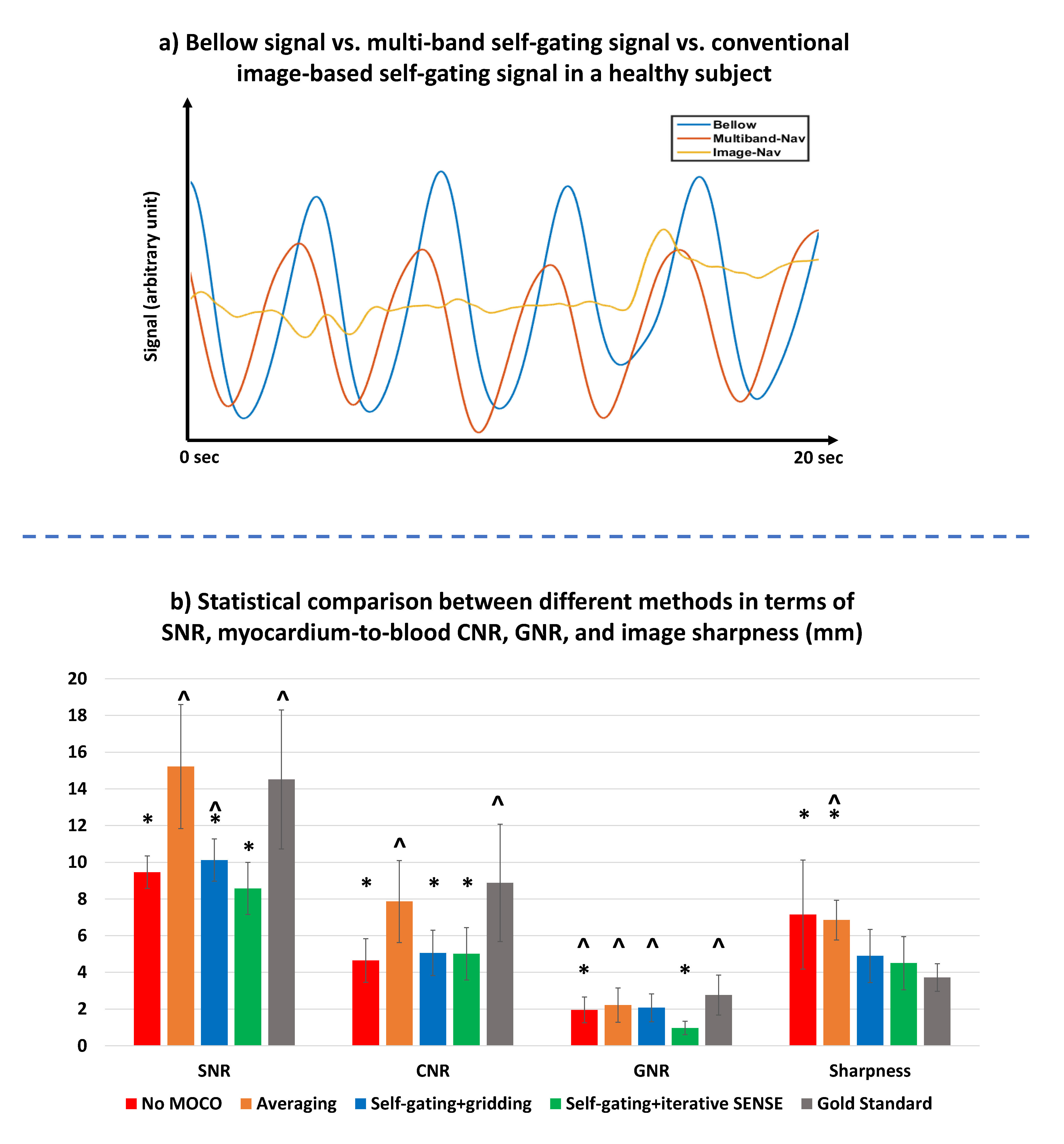
Data Analysis: The volumetric cine data was processed with 3 respiratory-gating approaches: no respiratory-gating, respiratory-correction with averaging, and respiratory-gating with the multi-band signal. Image SNR, blood-to-myocardium CNR, ghost-to-noise ratio (GNR), and image sharpness were evaluated for each motion-correction and reconstruction method, where the image sharpness was defined as the length of the image-intensity transition band from the myocardium to the blood pool in a mid-LV position.
Results
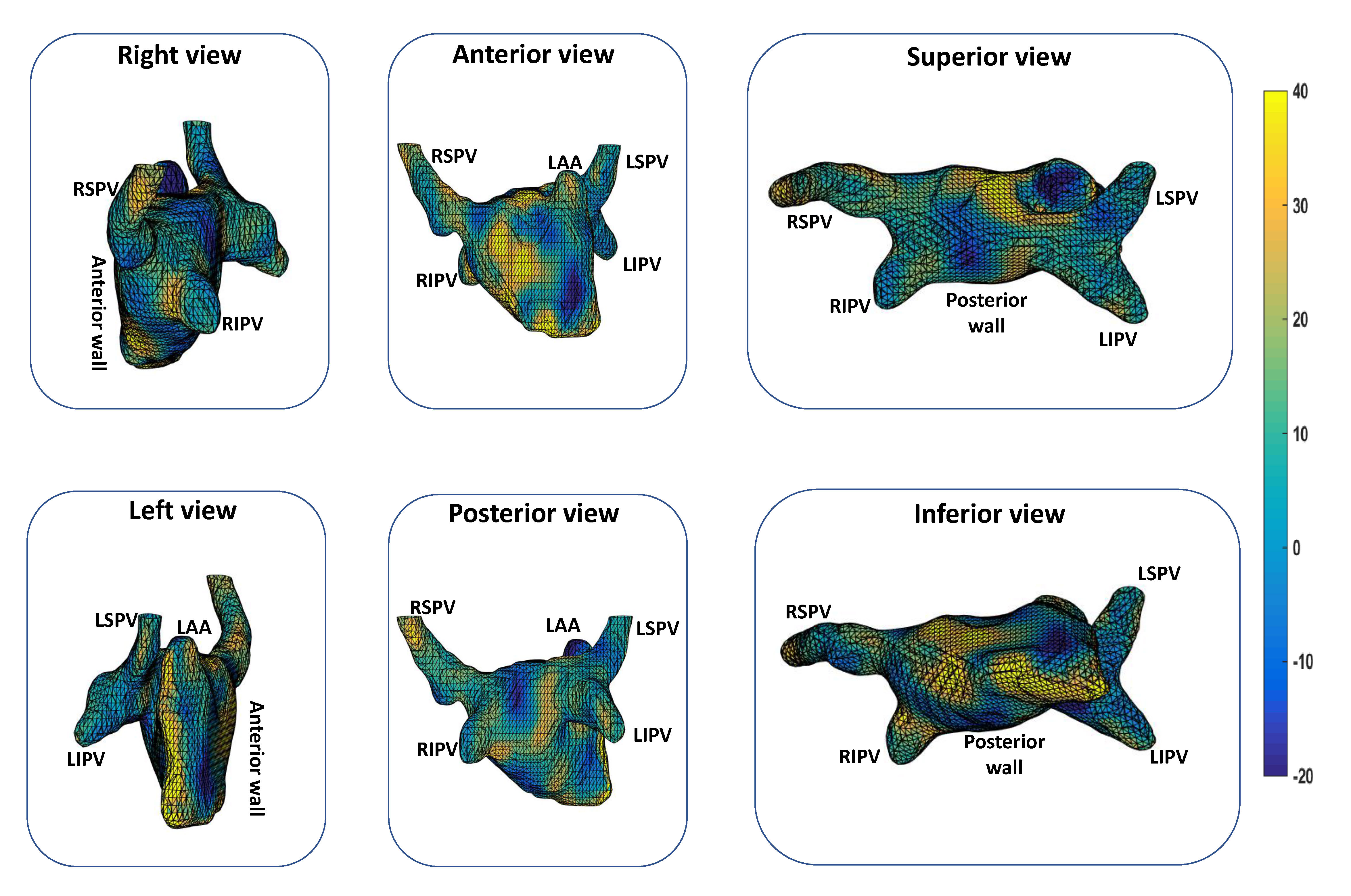
Figure 2 shows examples of the 3D cine image at mid-LA, reconstructed with different motion-correction methods, where the image quality was visually improved with the proposed multi-band gating method. The respiratory-bellow signal highly agrees with the multi-band self-gating signal (Figure 3a), with a 0.6-second delay that is consistent with previous reports (7). The traditional self-gating signal, however, fails to reliably show the breathing signal due to lack of motion information in the LA slice-plane. Figure 3b shows statistical comparison of image quality between different methods, where the proposed method had the lowest SNR (due to parallel imaging), but a better GNR and image sharpness than alternative motion-correction methods. Figure 4 shows an animation of the 3D strain maps from 4 healthy subjects and Figure 5 shows all 6 views of left atrium in one healthy subject. The average positive LA strain over healthy subjects was 19.5±2.7%.Conclusions
The results showed a stable performance using multi-band self-gating, and a sufficient image quality to generate a 3D strain map using feature tracking. There was a consistent LA strain pattern among the healthy subjects, e.g. the pulmonary vein ostia had a high positive strain. Comparison of the strain mapping with, for example, 3D left atrial gadolinium enhancement imaging of fibrosis might reveal a relationship, with low strain indicating stiffness.Acknowledgements
1. Evin et al, Assessment of Left Atrial Function by MRI Myocardial Feature Tracking, JMRI 2016
2. Peters et al, CMR-Verified Lower LA Strain in the Presence of Regional Atrial Fibrosis in Atrial Fibrillation, JACC Cardiovasc Imaging 2017
3. Nezafat et al, Inflow quantification in three‐dimensional cardiovascular MR imaging, JMRI 2008
4. Hu et al, Non-Contrast SSFP Pulmonary Vein MRA: Impact of Off-Resonance and Flow, JMRI 2011
5. Madore et al, Unaliasing by fourier-encoding the overlaps using the temporal dimension (UNFOLD), applied to cardiac imaging and fMRI, MRM 1999
6. Larson et al, Preliminary investigation of respiratory self-gating for free-breathing segmented cine MRI, MRM 2005
7. Liu et al, Respiratory and Cardiac Self-Gated Free-Breathing Cardiac CINE Imaging with Multi-Echo 3D Hybrid Radial SSFP Acquisition, MRM 2011
8. Rueckert et al, Nonrigid registration using free-form deformations: application to breast MR images, TMI 1999
References
Figures